
Optional statement
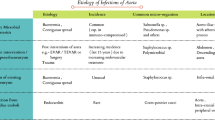
Infection of the aorta usually results from septic embolization to the vasa vasorum, hematogenous seeding of an existing aneurysm, or extension from a contiguous site of infection. The diagnosis should be considered in patients, often men over the age of 50 years with atherosclerosis, who present with fever, abdominal pain, palpable abdominal mass, and leukocytosis, with or without positive blood cultures. In the preantibiotic area, infectious aortitis was largely a complication of infective endocarditis, and was usually caused by group A streptococci, Streptococcus pneumoniae, or Haemophilus influenzae. Now a diverse array of bacteria and fungi has been associated, most commonly Salmonella species, which comprise nearly one third of the abdominal aortic infections and Staphylococcus aureus. Computed tomography is the most useful imaging modality. Medical treatment alone carries a high mortality, whereas the mortality with surgery combined with antimicrobial treatment is lower. Empiric antibiotics effective against S. aureus and gram-negative rods, such as Salmonella, should be initiated in cases identified before microbiologic diagnosis. Surgical débridement and revascularization should be completed early because delay may lead to aneurysm rupture, which increases mortality. The intent of surgery is to 1) control hemorrhage, if the aneurysm has ruptured; 2) confirm the diagnosis; 3) control sepsis; and 4) reconstruct the arterial vasculature. The patient should remain on parenteral or oral antibiotics for at least 6 weeks, perhaps longer, to assure full eradication of the pathogen and prevent recurrent infection. Close medical follow-up is indicated and includes serial blood cultures and computed tomography scans.
Similar content being viewed by others


References and Recommended Reading
Bronze MS, Shirwany A, Corbett CE, Schaberg DR: Infectious aortitis: an uncommon manifestation of infection with Streptococcus pneumoniae. Am J Med 1999, 107:627–630.
Oz MC, Brener BJ, Buda JA, et al.: A ten-year experience with bacterial aortitis. J Vasc Surg 1989, 10:439–449.
Osler W: The Gulstonian Lectures on malignant endocarditis. BMJ 1885, 1:467–470.
Macedo TA, Stanson AW, Oderich GS, et al.: Infected aortic aneurysms: imaging findings. Radiology 2004, 231:250–257.
Berchtold C, Eibl C, Seelig MH, et al.: Endovascular treatment and complete regression of an infected abdominal aortic aneurysm. J Endovasc Ther 2002, 9:543–548.
Fillmore AJ, Valentine RJ: Surgical mortality in patients with infected aortic aneurysms. J Am Coll Surg 2003, 196:435–441.
Muller BT, Wegener OR, Grabitz K, et al.: Mycotic aneurysms of the thoracic and abdominal aorta and iliac arteries: experience with anatomic and extra-anatomic repair in 33 cases. J Vasc Surg 2001, 33:106–113.
Reddy DJ, Ernst CB: Infected aneurysms. In Vascular Surgery.Edited by Rutherford RB. Philadelphia: WB Saunders;2000:1383–1397.
Oskoui R, Davis WA, Gomes MN: Salmonella aortitis. A report of a successfully treated case with a comprehensive review of the literature. Arch Intern Med 1993, 153:517–525.
Bayer AS, Scheld WM: Endocarditis and intravascular infections. In Principles and Practices of Infectious Diseases,edn 5. Edited by Mandell GL, et al. Philadelphia:Churchill Livingstone; 2000:857–902.
Guerrero F, Manuel L, Aguado JM, et al.: The spectrum of cardiovascular infections due to Salmonella enterica: a review of clinical features and factors determining outcome. Medicine (Baltimore) 2004, 83:123–128.
Soravia-Dunand VA, Loo VG, Salit IE: Aortitis due to Salmonella: report of 10 cases and comprehensive review of the literature. Clin Infect Dis 1999, 29:862–868.
Oz MC, McNicholas KW, Serra AJ, et al.: Review of Salmonella mycotic aneurysms of the thoracic aorta. J Cardiovasc Surg (Torino) 1989, 30:99–103.
Malouf JF, Chandrasekaran K, Orszulak TA: Mycotic aneurysms of the thoracic aorta: a diagnostic challenge. Am J Med 2003,115:489–496.
Ben-Haim S, Seabold JE, Hawes DR, Rooholamini SA: Leukocyte scintigraphy in the diagnosis of mycotic aneurysm. J Nucl Med 1992, 33:1486–1493.
Wein M, Bartel T, Kabatnik M, et al.: Rapid progression of bacterial aortitis to an ascending aortic mycotic aneurysm documented by transesophageal echocardiography. J Am Soc Echocardiogr 2001, 14:646–649.
Farkas JC, Fichelle JM, Laurian C, et al.: Long-term follow-up of positive cultures in 500 abdominal aortic aneurysms. Arch Surg 1993, 128:284–288.
van der Vliet JA, Kouwenberg PP, Muytjens HL, et al.: Relevance of bacterial cultures of abdominal aortic aneurysm contents. Surgery 1996, 119:129–132.
Vogt PR, Brunner-LaRocca HP, Lachat M, et al.: Technical details with the use of cryopreserved arterial allografts for aortic infection: influence on early and midterm mortality. J Vasc Surg 2002, 35:80–86.
Reddy DJ, Shepard AD, Evans JR, et al.: Management of infected aortoiliac aneurysms. Arch Surg 1991, 126:873–878; discussion 878–879.
Jarrett F, Darling C 3rd, Mundth ED, Austen WG: Experience with infected aneurysms of the abdominal aorta. Arch Surg 1975, 110:1281–1286.
Kryiakides C, Kan Y, Kerle M, et al.: 11-year experience with anatomical and extra-anatomical repair of mycotic aneurysms. Eur J Vasc Endovasc Surg 2004, 27:585–589.
Simon DR, Wishnow RM: An unusual presentation of salmonella aortitis. South Med J 1991, 84:657–659.
Gupta AK, Bandyk DF, Johnson BL: In situ repair of mycotic abdominal aortic aneurysms with rifampinbonded gelatin-impregnated Dacron grafts: a preliminary case report. J Vasc Surg 1996, 24:472–476.
Deglin JH, Vallerand AH: Davis’s Drug Guide, vol 6.0. Philadelphia: F.A. Davis Co.; 2003.
Chambers HF: Sulfonamides, trimethoprim and quinolones.In Basic and Clinical Pharmacology, edn 8.Edited by Katzung BG. St. Louis: Lange Medical Books/McGraw-Hill; 2001:793–802.
Delgado RM, Munoz-Bellido JL, Ibanez PR, et al.: Antimicrobial resistance in non-typhi Salmonellae in Castilla y Leon. Res Esp Quimioter 2004, 17:29–36.
Gomes MN, Choyke PL, Wallace RB: Infected aortic aneurysms. A changing entity. Ann Surg 1992, 215:435–442.
Pagni S, Denatale RW, Sweeney T, et al.: Primary aortoduodenal fistula secondary to infected abdominal aortic aneurysms: the role of local debridement and extra-anatomic bypass. J Cardiovasc Surg (Torino) 1999, 40:31–35.
Hsu RB, Tsay YG, Wang SS, Chu SH: Surgical treatment for primary infected aneurysm of the descending thoracic aorta, abdominal aorta, and iliac arteries. J Vasc Surg 2002, 36:746–750.
Luo CY, Ko WC, Kan CD, et al.: In situ reconstruction of septic aortic pseudoaneurysm due to Salmonella or Streptococcus microbial aortitis: long-term follow-up. J Vasc Surg 2003, 38:975–982.
Finseth FF, Abbott WM: One-stage operative therapy for Salmonella mycotic abdominal aortic aneurysm. Am Surg 1974, 179:8–11.
Cronenwett JL, Krupski WC, Rutherford RB: Abdominal aortic and iliac aneurysms. In Vascular Surgery, edn 5.Edited by Rutherford RB. Philadelphia: WB Saunders;2000:1246–1280.
Flamand F, Harris KA, DeRose G, et al.: Arteritis due to Salmonella with aneurysm formation: two cases. Can J Surg 1992, 35:248–252.
Leseche G, Castier Y, Petit MD, et al.: Long-term results of cryopreserved arterial allograft reconstruction in infected prosthetic grafts and mycotic aneurysms of the abdominal aorta. J Vasc Surg 2001, 34:616–622.
Teebken OE, Pichlmaier MA, Brand S, Haverich A: Cryopreserved arterial allografts for in situ reconstruction of infected arterial vessels. Eur J Vasc Endovasc Surg 2004, 27:597–602. Excellent report of a large series of patients with infectious aortitis or prosthetic graft infection managed with cryopreserved arterial homografts. Details the outcome and current issues with this procedure.
Semba CP, Sakai T, Slonim SM, et al.: Mycotic aneurysms of the thoracic aorta: repair with use of endovascular stent-grafts. J Vasc Interv Radiol 1998, 9(1Pt 1):33–40.
Ishida M, Kato N, Hirano T, et al.: Limitations of endovascular treatment with stent-grafts for active mycotic thoracic aortic aneurysm. Cardiovasc Intervent Radiol 2002, 25:216–218.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Foote, E.A., Postier, R.G., Greenfield, R.A. et al. Infectious Aortitis. Curr Treat Options Cardio Med 7, 89–97 (2005). https://doi.org/10.1007/s11936-005-0010-6
Issue Date:
DOI: https://doi.org/10.1007/s11936-005-0010-6