
Abstract
Recent studies have continued to examine the clinical associations of the group of autoantibodies that occurs predominantly in patients who have myositis (antibodies to aminoacyl-tRNA synthetases, to signal recognition particle [SRP], and to the nuclear helicase Mi-2). The antisynthetase syndrome has been further studied, and the value of tacrolimus in treatment of the associated interstitial lung disease has been noted. The low frequency of myositis specific autoantibodies in non-myositis neuromuscular disorders has been more clearly demonstrated. The clinical associations of anti-Mi-2 and anti-SRP were further studied, and patients with antibodies without myositis were reported. Evidence suggested that ultraviolet light exposure may influence the expression of dermatomyositis and anti-Mi-2. A new classification for myositis using overlap clinical features and autoantibodies was proposed. A new autoantibody, anti-caDM-140, was described, associated with clinically amyopathic dermatomyositis and interstitial lung disease. The possibility was raised that increased antigen expression in regenerating muscle may help to perpetuate the disease. These antibodies continue to be the subject of active investigation.
Similar content being viewed by others

References and Recommended Reading
Love LA, Leff RL, Fraser DD, et al.: A new approach to the classification of idiopathic inflammatory myopathy: myositis-specific autoantibodies define useful homogeneous patient groups. Medicine 1991, 70:360–374.
Casciola-Rosen LA, Pluta AF, Plotz PH, et al.: The DNA mismatch repair enzyme PMS1 is a myositis-specific autoantigen. Arthritis Rheum 2001, 44:389–396.
Sato S, Hirakata M, Kuwana M, et al.: Autoantibodies to a 140-kd polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum 2005, 52:1571–1576. Description of a significant new autoantibody associated with amyopathic DM, particularly the subset common in Asian patients that has a high risk of severe ILD. This subgroup has a low frequency of other autoantibodies.
Williams J, Lucas M, Fertig N, Medsger TA: Anti-Ku antibody in patients with systemic sclerosis: comparison of clinical features associated with anti-U1RNP, anti- U3RNP, and anti-PM-Scl antibodies [abstract]. Arthritis Rheum 2005, 52:S590-S591.
Jablonska S, Blaszyk M: Scleromyositis (scleroderma/ polimyositis overlap) is an entity. J Eur Acad Dermatol Venereol 2004, 18:265–266.
Targoff IN: Idiopathic inflammatory myopathy: autoantibody update. Curr RheumatolRep 2002, 4:434–441.
Targoff IN: Laboratory testing in the diagnosis and management of idiopathic inflammatory myopathies. Rheum Dis Clin North Am 2002, 28:859–890.
Hengstman GJ, van Engelen BG, van Venrooij WJ: Myositis specific autoantibodies: changing insights in pathophysiology and clinical associations. Curr Opin Rheumatol 2004, 16:692–699.
Arnett FC, Targoff IN, Mimori T, et al.: Interrelationship of major histocompatibility complex class II alleles and autoantibodies in four ethnic groups with various forms of myositis. Arthritis Rheum 1996, 39:1507–1518.
Schmidt WA, Wetzel W, Friedlander R, et al.: Clinical and serological aspects of patients with anti-Jo-1 antibodies—an evolving spectrum of disease manifestations. Clin Rheumatol 2000, 19:371–377.
Hengstman GJ, Brouwer R, Egberts WT, et al.: Clinical and serological characteristics of 125 Dutch myositis patients. Myositis specific autoantibodies aid in the differential diagnosis of the idiopathic infiammatory myopathies. J Neurol 2002, 249:69–75.
Chinoy H, Salway F, Fertig N, et al.: In adult onset myositis, the presence of interstitial lung disease and myositis specific/associated antibodies are governed by HLA class II haplotype, rather than by myositis subtype. Arthritis Res Ther 2006, 8:R13. A large multicenter study of immunogenetics of myositis in the UK, noted significant associations with ILD even in anti-aaRSnegative patients, suggesting a potential primary association of HLA with this manifestation rather than through the antibody.
Brouwer R, Hengstman GJ, Vree Egberts W, et al.: Autoantibody profiles in the sera of European patients with myositis. Ann Rheum Dis 2001, 60:116–123.
Marie I, Hachulla E, Cherin P, et al.: Interstitial lung disease in polymyositis and dermatomyositis. Arthritis Rheum 2002, 47:614–622.
Furuya T, Hakoda M, Tsuchiya N, et al.: Immunogenetic features in 120 Japanese patients with idiopathic inflammatory myopathy. J.Rheumatol 2004, 31:1768–1774. Association of HLA type with myositis and with anti-aaRS showed differences from risk factors for whites.
Wilkes MR, Sereika SM, Fertig N, et al.: Treatment of antisynthetase-associated interstitial lung disease with tacrolimus. Arthritis Rheum 2005, 52:2439–2446. Although retrospective, there appeared to be an important therapeutic effect and tacrolimus may be a valuable option for the lung disease as well as for the myositis. Forced vital capacity, FEV1, and diffusing capacity all showed improvement.
Spath M, Schroder M, Schlotter-Weigel B, et al.: The long-term outcome of anti-Jo-1-positive inflammatory myopathies. J Neurol 2004, 251:859–864. There is limited data concerning prognosis in anti-Jo-1 patients. Although there was one fatality from progressive ILD, there was stabilization of ILD and improvement of myositis in most, but most needed to continue immunosuppressive treatment.
Fathi M, Dastmalchi M, Rasmussen E, et al.: Interstitial lung disease, a common manifestation of newly diagnosed polymyositis and dermatomyositis. Ann Rheum Dis 2004, 63:297–301. ILD was common in myositis when sensitive tests were used, even in anti-Jo-1 negative patients. This suggests that the frequency may be higher than recognized.
Friedman AW, Targoff IN, Arnett FC: Interstitial lung disease with autoantibodies against aminoacyl-tRNA synthetases in the absence of clinically apparent myositis. Semin Arthritis Rheum 1996, 26:459–467.
Sato S, Hirakata M, Kuwana M, et al.: Clinical characteristics of Japanese patients with anti-PL-7 (anti-threonyl-tRNA synthetase) autoantibodies. Clin Exp Rheumatol 2005, 23:609–615. Only a limited number of patients with anti-PL-7 have been described, although the clinical picture remains similar to other anti-aaRS patients. One of seven had ILD without myositis. Arthritis (six of seven patients) and SSc overlap (five of seven) were common, with the latter including some diffuse cutaneous involvement, unusual with anti-aaRS.
Kao AH, Lacomis D, Lucas M, et al.: Anti-signal recognition particle autoantibody in patients with and patients without idiopathic inflammatory myopathy. Arthritis Rheum 2004, 50:209–215. A review of a relatively large experience with anti-SRP-associated myopathy. This group frequently has severe disease and sometimes has disease that is difficult to treat. They can sometimes have a confusing picture by biopsy due to the paucity of indflammation. Available information on this group in the literature is limited.
Yamasaki Y, Narain S, Hernandez L, et al.: Myositis-related autoantibodies in patients with elevated CPK or interstitial lung disease without diagnosis of PM/DM [abstract]. Arthritis Rheum 2005, 52:S312.
Sato S, Kaneko Y, Asano K, et al.: Clinical and immunological characteristics in Japanese patients with idiopathic interstitial pneumonias [abstract]. Arthritis Rheum 2005, 52:S245.
Fathi M, Lundberg IE: Interstitial lung disease in polymyositis and dermatomyositis. Curr Opin Rheumatol 2005, 17:701–706.
Joffe MM, Love LA, Leff RL, et al.: Drug therapy of the idiopathic inflammatory myopathies: predictors of response to prednisone, azathioprine, and methotrexate and a comparison of their efficacy. Am J Med 1993, 94:379–387.
Cronin ME, Miller FW, Hicks JE, et al.: The failure of intravenous cyclophosphamide therapy in refractory idiopathic inflammatory myopathy. J Rheumatol 1989, 16:1225–1228.
Mozaffar T, Pestronk A: Myopathy with anti-Jo-1 antibodies: pathology in perimysium and neighbouring muscle.bres. J Neurol Neurosurg Psychiatry 2000, 68:472–478.
Targoff IN, Reichlin M: The association between Mi-2 antibodies and dermatomyositis. Arthritis Rheum 1985, 28:796–803.
Mierau R, Dick T, Bartz-Bazzanella P, et al.: Strong association of dermatomyositis-specific Mi-2 autoantibodies with a tryptophan at position 9 of the HLA-DR beta chain. Arthritis Rheum 1996, 39:868–876.
Hausmanowa-Petrusewicz I, Kowalska-Oledzka E, Miller FW, et al.: Clinical, serologic, and immunogenetic features in Polish patients with idiopathic inflammatory myopathies. Arthritis Rheum 1997, 40:1257–1266.
Hengstman GJ, Vree Egberts WT, Seelig HP, et al.: Clinical characteristics of patients with myositis and autoantibodies to different fragments of the Mi-2 antigen. Ann Rheum Dis 2006, 65:242–245. Study of a large number of European patients with anti-Mi-2 by ELISA. Almost as many patients had PM as DM (40% vs 50%), a markedly different result from IPP studies [12], and some difference from ELISA studies with confirmation by blotting [13]. Disease was considered generally milder with more complete responses. More CAM patients reacted with the N-terminal, though not significant. Clinical associations may not be applicable to the blot-confirmed or IPP/immunodiffusion anti-Mi-2 group [1, 28–30]. It would be of interest to further characterize the antibody activity that represents the differences between these groups, since it may have its own clinical associations.
Watkins J, Farzaneh-Far R, Tahir H, et al.: Jo-1 syndrome with associated poorly differentiated adenocarcinoma. [Review] [5 refs]. Rheumatology 2004, 43:389–390.
Hengstman GJ, van Brenk L, Vree Egberts WT, et al.: High specificity of myositis specific autoantibodies for myositis compared with other neuromuscular disorders. J Neurol 2005, 252:534–537. An important confirmation of previous impressions regarding the disease specificity of MSAs. Although neuromuscular disorders are often the main alternative diagnoses in patients being evaluated for myositis, most control groups for MSA studies have been rheumatic diseases. One patient with mitochondrial myopathy had blot-confirmed anti-Mi-2; although this represents only a small percentage of those tested, it could be significant and was not seen with anti-Jo-1. Further testing is needed to determine if this is representative.
Nagaraju K, Raben N, Loeffier L, et al.: Conditional up-regulation of MHC class I in skeletal muscle leads to self-sustaining autoimmune myositis and myositisspeci.c autoantibodies. Proc Natl Acad Sci U S A 2000, 97:9209–9214.
Ge Q, Nilasena DS, O’Brien CA, et al.: Molecular analysis of a major antigenic region of the 240-kD protein of Mi-2 autoantigen. J Clin Invest 1995, 96:1730–1737.
Okada S, Weatherhead E, Targoff IN, et al.: Global surface ultraviolet radiation intensity may modulate the clinical and immunologic expression of autoimmune muscle disease. Arthritis Rheum 2003, 48:2285–2293.
Casciola-Rosen L, Andrade F, Ulanet D, et al.: Cleavage by granzyme B is strongly predictive of autoantigen status: implications for initiation of autoimmunity. J Exp Med 1999, 190:815–826.
Targoff IN, Johnson AE, Miller FW: Antibody to signal recognition particle in polymyositis. Arthritis Rheum 1990, 33:1361–1370.
Miller T, Al Lozi MT, Lopate G, Pestronk A: Myopathy with antibodies to the signal recognition particle: clinical and pathological features. J Neurol Neurosurg Psychiatry 2002, 73:420–428.
Römisch K, Miller FW, Dobberstein B, High S: Human autoantibodies against the 54 kDa protein of the signal recognition particle block function at multiple stages. Arthritis Res Ther 2006, 8:R39. An elegant and detailed demonstration of the effects of autoantibodies to the SRP 54kd protein on SRP function. Information regarding epitope reactivity of SRP54 was provided.
Hirakata M, Matsuura Y, Suwa A, et al.: Immunological and histopathological features of patients with anti-SRP autoantibodies [abstract]. Arthritis Rheum 1997, 40.
Satoh T, Okano T, Matsui T, et al.: Novel autoantibodies against 7SL RNA in patients with polymyositis/dermatomyositis. J Rheumatol 2005, 32:1727–1733. Autoantibodies reacting directly with the 7SL RNA of the signal recognition particle occur in some patients with anti-SRP. The.nding that a portion of sera with an autoantibody to a protein also react with an associated RNA has been previously observed (anti-Jo-1 [13], anti-U1RNP, and so on), suggesting epitope spreading. The frequency of anti-7SL differed in Japanese and US patients, and there were associated clinical differences in anti-7SL positive versus negative anti-SRP patients, such as proportion of DM.
Leff RL, Burgess SH, Miller FW, et al.: Distinct seasonal patterns in the onset of adult idiopathic inflammatory myopathy in patients with anti-Jo-1 and anti-signal recognition particle autoantibodies. Arthritis Rheum 1991, 34:1391–1396.
Sarkar K, Weinberg CR, Oddis CV, et al.: Seasonal influence on the onset of idiopathic inflammatory myopathies in serologically defined groups. Arthritis Rheum 2005, 52:2433–2438. Seasonal onset suggests possible environmental triggers. The original observations [42] regarding anti-SRP could not be confirmed in this larger, multicenter study, but a subgroup of anti-synthetase-associated myositis was more likely to have onset in the Spring. Since some subgroups have low frequency, future study may still reveal important seasonal associations in particular subgroups or geographical areas.
Ge Q, Wu Y, Trieu EP, Targoff IN: Analysis of fine specificity of anti-PM-Scl autoantibodies. Arthritis Rheum 1994, 37:1445–1452.
Alderuccio F, Barnett AJ, Campbell JH, et al.: Scl-95/100: doublet of endothelial marker autoantigens in progressive systemc sclerosis. Clin Exp Immunol 1986, 64:94–100.
Brouwer R, Vree Egberts WT, Hengstman GJ, et al.: Autoantibodies directed to novel components of the PM/Scl complex, the human exosome. Arthritis Res 2002, 4:134–138.
Raijmakers R, Renz M, Wiemann C, et al.: PM-Scl-75 is the main autoantigen in patients with the polymyositis/ scleroderma overlap syndrome. Arthritis Rheum 2004, 50:565–569. Earlier studies of reaction with recombinant PMScl-75 protein used a form that appears to be incomplete, and this study with full-length protein showed more frequent reaction. However, previous blotting studies of natural PM-Scl also showed lower PMScl-75 than PMScl-100 reaction. Further study is needed to confirm specificity.
Mahler M, Raijmakers R, Dahnrich C, et al.: Clinical evaluation of autoantibodies to a novel PM/Scl peptide antigen. Arthritis Res Ther 2005, 7:R704-R713. This is an interesting study of a new ELISA, but there appeared to be wider reactivity than usual anti-PM-Scl testing, including a small percent of control sera. The high sensitivity suggested use for screening with subsequent confirmatory tests.
Schnitz W, Taylor-Albert E, Targoff IN, et al.: Anti-PM/Scl autoantibodies in patients without clinical polymyositis or scleroderma. J Rheumatol 1996, 23:1729–1733.
Warner NZ, Greidinger EL: Patients with antibodies to both PmScl and dsDNA. J Rheumatol 2004, 31:2169–2174.
Marguerie C, Bunn CC, Copier J, et al.: The clinical and immunogenetic features of patients with autoantibodies to the nucleolar antigen PM-Scl. Medicine 1992, 71:327–336.
Reichlin M, Maddison PJ, Targoff IN, et al.: Antibodies to a nuclear/nucleolar antigen in patients with polymyositisoverlap syndrome. J Clin Immunol 1984, 4:40–44.
van der Meulen MF, Bronner IM, Hoogendijk JE, et al.: Polymyositis: an overdiagnosed entity. Neurology 2003, 61:316–321.
Troyanov Y, Targoff IN, Tremblay JL, et al.: Novel classification of idiopathic infiammatory myopathies based on overlap syndrome features and autoantibodies: analysis of 100 French Canadian patients. Medicine 2005, 84:231–249. A suggestion for a revision of classification criteria based on a detailed analysis of a large myositis population. Including all patients with any connective tissue disease feature or related autoantibody in the connective tissue disease-myositis group results in a pure PM group that is smaller, less treatment-responsive, but potentially more homogeneous.
Shamim EA, Rider LG, Pandey JP, et al.: Differences in idiopathic inflammatory myopathy phenotypes and genotypes between Mesoamerican Mestizos and North American Caucasians: ethnogeographic influences in the genetics and clinical expression of myositis. Arthritis Rheum 2002, 46:1885–1893.
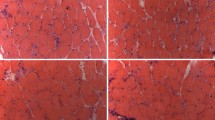
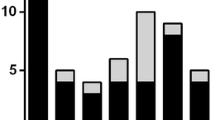
Casciola-Rosen L, Nagaraju K, Plotz P, et al.: Enhanced autoantigen expression in regenerating muscle cells in idiopathic inflammatory myopathy. J Exp Med 2005, 201:591–601. An interesting study suggesting that overexpression of myositis antigens in regenerating muscle fibers may be the source of the continuing autoimmune response against the muscle. The finding that anti-Mi-2 was overexpressed only in DM muscle is of particular note, significantly strengthening the impression that this overexpression is pathogenetically important.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Targoff, I.N. Myositis specific autoantibodies. Curr Rheumatol Rep 8, 196–203 (2006). https://doi.org/10.1007/s11926-996-0025-3
Issue Date:
DOI: https://doi.org/10.1007/s11926-996-0025-3