
Abstract
Purpose of Review
The review aims to summarize our current knowledge surrounding treatment strategies aimed at recovery of bone mass in energy-deficient women suffering from the Female Athlete Triad.
Recent Findings
The independent and interactive contributions of energy status versus estrogen status on bone density, geometry, and strength have recently been reported, highlighting the importance of addressing both energy and estrogen in treatment strategies for bone health. This is supported by reports that have identified energy-related features (low body weight and BMI) and estrogen-related features (late age of menarche, oligo/amenorrhea) to be significant risk factors for low bone mineral density and bone stress injury in female athletes and exercising women.
Summary
Nutritional therapy is the recommended first line of treatment to recover bone mass in energy-deficient female athletes and exercising women. If nutritional therapy fails after 12 months or if fractures or significant worsening in BMD occurs, pharmacological therapy may be considered in the form of transdermal estradiol with cyclic oral progestin (not COC).

Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Weaver CM, Gordon CM, Janz KF, Kalkwarf HJ, Lappe JM, Lewis R, et al. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int: J Established Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 2016;27(4):1281–386. doi:10.1007/s00198-015-3440-3.
Golden NH, Abrams SA. Optimizing bone health in children and adolescents. Pediatrics. 2014;134(4):e1229–43. doi:10.1542/peds.2014-2173.
Baxter-Jones AD, Faulkner RA, Forwood MR, Mirwald RL, Bailey DA. Bone mineral accrual from 8 to 30 years of age: an estimation of peak bone mass. J Bone Miner Res. 2011;26(8):1729–39. doi:10.1002/jbmr.412.
•• De Souza MJ, Nattiv A, Joy E, Misra M, Williams NI, Mallinson RJ, et al. Female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, CA, May 2012, and 2nd international conference held in Indianapolis, IN, May 2013. Clin J Sport Med. 2014;24(2):96–119. doi:10.1097/JSM.0000000000000085. This consensus statement, composed by an international, multidisciplinary team of scientists and clinicians comprising the Female Athlete Triad Coalition, is the only resource published to date that relies on current evidence-based knowledge to offer specific recommendations for the screening, diagnosis, and treatment, as well as detailed return to play guidelines for the Female Athlete Triad.
•• De Souza MJ, Nattiv A, Joy E, Misra M, Williams NI, Mallinson RJ, et al. Female athlete triad coalition consensus statement on treatment and return to play of the female athlete triad: 1st international conference held in San Francisco, California, May 2012 and 2nd international conference held in Indianapolis, Indiana, May 2013. Br J Sports Med. 2014;48(4):289. doi:10.1136/bjsports-2013-093218. This consensus statement, composed by an international, multidisciplinary team of scientists and clinicians comprising the Female Athlete Triad Coalition, is the only resource published to date that relies on current evidence-based knowledge to offer specific recommendations for the screening, diagnosis, and treatment, as well as detailed return to play guidelines for the Female Athlete Triad.
Matkovic V, Jelic T, Wardlaw GM, Ilich JZ, Goel PK, Wright JK, et al. Timing of peak bone mass in Caucasian females and its implication for the prevention of osteoporosis. Inference from a cross-sectional model. J Clin Invest. 1994;93(2):799–808. doi:10.1172/JCI117034.
Clarke BL, Khosla S. Physiology of bone loss. Radiol Clin N Am. 2010;48(3):483–95. doi:10.1016/j.rcl.2010.02.014.
Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P, et al. Predictive value of BMD for hip and other fractures. J Bone Miner Res. 2005;20(7):1185–94. doi:10.1359/JBMR.050304.
Yeager KK, Agostini R, Nattiv A, Drinkwater B. The female athlete triad: disordered eating, amenorrhea, osteoporosis. Med Sci Sports Exerc. 1993;25(7):775–7.
Nattiv A, Loucks AB, Manore MM, Sanborn CF, Sundgot-Borgen J, Warren MP. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867–82. doi:10.1249/mss.0b013e318149f111.
Wade GN, Schneider JE. Metabolic fuels and reproduction in female mammals. Neurosci Biobehav Rev. 1992;16(2):235–72.
Weitzmann MN, Pacifici R. Estrogen deficiency and bone loss: an inflammatory tale. J Clin Invest. 2006;116(5):1186–94. doi:10.1172/JCI28550.
Drinkwater BL, Bruemner B, Chesnut CH 3rd. Menstrual history as a determinant of current bone density in young athletes. JAMA. 1990;263(4):545–8.
Keen AD, Drinkwater BL. Irreversible bone loss in former amenorrheic athletes. Osteoporos Int. 1997;7(4):311–5.
Warren MP, Brooks-Gunn J, Fox RP, Holderness CC, Hyle EP, Hamilton WG, et al. Persistent osteopenia in ballet dancers with amenorrhea and delayed menarche despite hormone therapy: a longitudinal study. Fertil Steril. 2003;80(2):398–404.
Drinkwater BL, Nilson K, Chesnut CH 3rd, Bremner WJ, Shainholtz S, Southworth MB. Bone mineral content of amenorrheic and eumenorrheic athletes. N Engl J Med. 1984;311(5):277–81. doi:10.1056/NEJM198408023110501.
Cobb KL, Bachrach LK, Greendale G, Marcus R, Neer RM, Nieves J, et al. Disordered eating, menstrual irregularity, and bone mineral density in female runners. Med Sci Sports Exerc. 2003;35(5):711–9. doi:10.1249/01.MSS.0000064935.68277.E7.
Marcus R, Cann C, Madvig P, Minkoff J, Goddard M, Bayer M, et al. Menstrual function and bone mass in elite women distance runners. Endocrine and metabolic features. Ann Intern Med. 1985;102(2):158–63.
Myburgh KH, Bachrach LK, Lewis B, Kent K, Marcus R. Low bone mineral density at axial and appendicular sites in amenorrheic athletes. Med Sci Sports Exerc. 1993;25(11):1197–202.
Nichols JF, Rauh MJ, Barrack MT, Barkai HS. Bone mineral density in female high school athletes: interactions of menstrual function and type of mechanical loading. Bone. 2007;41(3):371–7. doi:10.1016/j.bone.2007.05.003.
Mallinson RJ, Williams NI, Hill BR, De Souza MJ. Body composition and reproductive function exert unique influences on indices of bone health in exercising women. Bone. 2013;56(1):91–100. doi:10.1016/j.bone.2013.05.008.
• Mallinson RJ, Williams NI, Gibbs JC, Koehler K, Allaway HC, Southmayd E, et al. Current and past menstrual status is an important determinant of femoral neck geometry in exercising women. Bone. 2016;88:101–12. doi:10.1016/j.bone.2016.01.030. Building upon the classic work of Dr. Drinkwater, this study described the cumulative effect of current and past menstrual irregularity on femoral neck geometry, highlighting the persistent and significant detriment of estrogen deficiency on bone strength estimates.
Ackerman KE, Pierce L, Guereca G, Slattery M, Lee H, Goldstein M, et al. Hip structural analysis in adolescent and young adult oligoamenorrheic and eumenorrheic athletes and nonathletes. J Clin Endocrinol Metab. 2013;98(4):1742–9. doi:10.1210/jc.2013-1006.
Ackerman KE, Nazem T, Chapko D, Russell M, Mendes N, Taylor AP, et al. Bone microarchitecture is impaired in adolescent amenorrheic athletes compared with eumenorrheic athletes and nonathletic controls. J Clin Endocrinol Metab. 2011;96(10):3123–33. doi:10.1210/jc.2011-1614.
Ducher G, Eser P, Hill B, Bass S. History of amenorrhoea compromises some of the exercise-induced benefits in cortical and trabecular bone in the peripheral and axial skeleton: a study in retired elite gymnasts. Bone. 2009;45(4):760–7. doi:10.1016/j.bone.2009.06.021.
Beck TJ. Extending DXA beyond bone mineral density: understanding hip structure analysis. Curr Osteoporos Rep. 2007;5(2):49–55.
Beck TJ, Broy SB. Measurement of hip geometry-technical background. J Clin Densitom. 2015;18(3):331–7. doi:10.1016/j.jocd.2015.06.006.
Ackerman KE, Putman M, Guereca G, Taylor AP, Pierce L, Herzog DB, et al. Cortical microstructure and estimated bone strength in young amenorrheic athletes, eumenorrheic athletes and non-athletes. Bone. 2012;51(4):680–7. doi:10.1016/j.bone.2012.07.019.
Chevalley T, Bonjour JP, van Rietbergen B, Rizzoli R, Ferrari S. Fractures in healthy females followed from childhood to early adulthood are associated with later menarcheal age and with impaired bone microstructure at peak bone mass. J Clin Endocrinol Metab. 2012;97(11):4174–81. doi:10.1210/jc.2012-2561.
Ackerman KE, Cano Sokoloff N, Denm G, Clarke HM, Lee H, Misra M. Fractures in relation to menstrual status and bone parameters in young athletes. Med Sci Sports Exerc. 2015;47(8):1577–86. doi:10.1249/MSS.0000000000000574.
Wentz L, Liu PY, Haymes E, Ilich JZ. Females have a greater incidence of stress fractures than males in both military and athletic populations: a systemic review. Mil Med. 2011;176(4):420–30.
Bennell KL, Malcolm SA, Thomas SA, Wark JD, Brukner PD. The incidence and distribution of stress fractures in competitive track and field athletes. A twelve-month prospective study. Am J Sports Med. 1996;24(2):211–7. doi:10.1177/036354659602400217.
• Barrack MT, Gibbs JC, De Souza MJ, Williams NI, Nichols JF, Rauh MJ, et al. Higher incidence of bone stress injuries with increasing female athlete triad-related risk factors: a prospective multisite study of exercising girls and women. Am J Sports Med. 2014;42(4):949–58. doi:10.1177/0363546513520295. This investigation uniquely described the effect of a single Triad risk factor and combinations of 2 and 3 Triad risk factors on the incidence of bone stress injuries in exercising adolescent girls and women, thereby informing evidence-based clinical assessment of injury risk in this population.
Kadel NJ, Teitz CC, Kronmal RA. Stress fractures in ballet dancers. Am J Sports Med. 1992;20(4):445–9. doi:10.1177/036354659202000414.
Warren MP, Brooks-Gunn J, Hamilton LH, Warren LF, Hamilton WG. Scoliosis and fractures in young ballet dancers. Relation to delayed menarche and secondary amenorrhea. N Engl J Med. 1986;314(21):1348–53. doi:10.1056/NEJM198605223142104.
Bennell KL, Malcolm SA, Thomas SA, Ebeling PR, McCrory PR, Wark JD, et al. Risk factors for stress fractures in female track-and-field athletes: a retrospective analysis. Clin J Sport Med. 1995;5(4):229–35.
Carbon R, Sambrook PN, Deakin V, Fricker P, Eisman JA, Kelly P, et al. Bone density of elite female athletes with stress fractures. Med J Aust. 1990;153(7):373–6.
Duckham RL, Peirce N, Meyer C, Summers GD, Cameron N, Brooke-Wavell K. Risk factors for stress fracture in female endurance athletes: a cross-sectional study. BMJ Open. 2012;2(6):e001920. https://doi.org/10.1136/bmjopen-2012-001920.
Myburgh KH, Hutchins J, Fataar AB, Hough SF, Noakes TD. Low bone density is an etiologic factor for stress fractures in athletes. Ann Intern Med. 1990;113(10):754–9.
Nattiv A, Kennedy G, Barrack MT, Abdelkerim A, Goolsby MA, Arends JC, et al. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: a 5-year prospective study in collegiate track and field athletes. Am J Sports Med. 2013;41(8):1930–41. doi:10.1177/0363546513490645.
Hergenroeder AC, Smith EO, Shypailo R, Jones LA, Klish WJ, Ellis K. Bone mineral changes in young women with hypothalamic amenorrhea treated with oral contraceptives, medroxyprogesterone, or placebo over 12 months. Am J Obstet Gynecol. 1997;176(5):1017–25.
Warren MP, Miller KK, Olson WH, Grinspoon SK, Friedman AJ. Effects of an oral contraceptive (norgestimate/ethinyl estradiol) on bone mineral density in women with hypothalamic amenorrhea and osteopenia: an open-label extension of a double-blind, placebo-controlled study. Contraception. 2005;72(3):206–11. doi:10.1016/j.contraception.2005.03.007.
Rickenlund A, Carlstrom K, Ekblom B, Brismar TB, Von Schoultz B, Hirschberg AL. Effects of oral contraceptives on body composition and physical performance in female athletes. J Clin Endocrinol Metab. 2004;89(9):4364–70. doi:10.1210/jc.2003-031334.
Grinspoon SK, Friedman AJ, Miller KK, Lippman J, Olson WH, Warren MP. Effects of a triphasic combination oral contraceptive containing norgestimate/ethinyl estradiol on biochemical markers of bone metabolism in young women with osteopenia secondary to hypothalamic amenorrhea. J Clin Endocrinol Metab. 2003;88(8):3651–6. doi:10.1210/jc.2003-030033.
Cobb KL, Bachrach LK, Sowers M, Nieves J, Greendale GA, Kent KK, et al. The effect of oral contraceptives on bone mass and stress fractures in female runners. Med Sci Sports Exerc. 2007;39(9):1464–73. doi:10.1249/mss.0b013e318074e532.
Cumming DC. Exercise-associated amenorrhea, low bone density, and estrogen replacement therapy. Arch Intern Med. 1996;156(19):2193–5.
Klibanski A, Biller BM, Schoenfeld DA, Herzog DB, Saxe VC. The effects of estrogen administration on trabecular bone loss in young women with anorexia nervosa. J Clin Endocrinol Metab. 1995;80(3):898–904. doi:10.1210/jcem.80.3.7883849.
Carlson JL, Curtis M, Halpern-Felsher B. Clinician practices for the management of amenorrhea in the adolescent and young adult athlete. J Adolesc Health. 2007;40(4):362–5. doi:10.1016/j.jadohealth.2006.10.017.
De Souza MJ, West SL, Jamal SA, Hawker GA, Gundberg CM, Williams NI. The presence of both an energy deficiency and estrogen deficiency exacerbate alterations of bone metabolism in exercising women. Bone. 2008;43(1):140–8. doi:10.1016/j.bone.2008.03.013S8756-3282(08)00166-X.
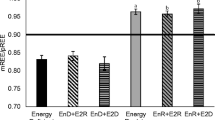
• Southmayd EA, Mallinson RJ, Williams NI, Mallinson DJ, De Souza MJ. Unique effects of energy versus estrogen deficiency on multiple components of bone strength in exercising women. Osteoporos Int. 2017;28(4):1365–76. doi:10.1007/s00198-016-3887-x. This is the first study to isolate the contribution of energy status versus estrogen status on volumetric bone mineral density, bone geometry, and estimated bone strength in exercising women with and without menstrual disturbances.
• Gibbs JC, Nattiv A, Barrack MT, Williams NI, Rauh MJ, Nichols JF, et al. Low bone density risk is higher in exercising women with multiple triad risk factors. Med Sci Sports Exerc. 2014;46(1):167–76. doi:10.1249/MSS.0b013e3182a03b8b. This investigation uniquely described the effect of a single Triad risk factor and a combination of 2 and 3 Triad risk factors on bone health, identifying specific energetic and menstrual factors that are associated with low bone mineral density in exercising adolescent girls and women.
Loucks AB. Energy availability and infertility. Curr Opin Endocrinol Diabetes Obes. 2007;14(6):470–4. doi:10.1097/MED.0b013e3282f1cb6a.
Loucks AB, Thuma JR. Luteinizing hormone pulsatility is disrupted at a threshold of energy availability in regularly menstruating women. J Clin Endocr Metab. 2003;88(1):297–311. doi:10.1210/jc.2002-020369.
Loucks AB, Verdun M, Heath EM. Low energy availability, not stress of exercise, alters LH pulsatility in exercising women. J Appl Physiol. 1998;84(1):37–46.
Dueck CA, Matt KS, Manore MM, Skinner JS. Treatment of athletic amenorrhea with a diet and training intervention program. Int J Sport Nutr. 1996;6(1):24–40.
Kopp-Woodroffe SA, Manore MM, Dueck CA, Skinner JS, Matt KS. Energy and nutrient status of amenorrheic athletes participating in a diet and exercise training intervention program. Int J Sport Nutr. 1999;9(1):70–88.
Mallinson RJ, Williams NI, Olmsted MP, Scheid JL, Riddle ES, De Souza MJ. A case report of recovery of menstrual function following a nutritional intervention in two exercising women with amenorrhea of varying duration. J Int Soc Sports Nutr. 2013;10:34. doi:10.1186/1550-2783-10-34.
Ihle R, Loucks AB. Dose-response relationships between energy availability and bone turnover in young exercising women. J Bone Miner Res. 2004;19(8):1231–40. doi:10.1359/JBMR.040410.
Miller KK, Lee EE, Lawson EA, Misra M, Minihan J, Grinspoon SK, et al. Determinants of skeletal loss and recovery in anorexia nervosa. J Clin Endocrinol Metab. 2006;91(8):2931–7. doi:10.1210/jc.2005-2818.
Lindberg JS, Powell MR, Hunt MM, Ducey DE, Wade CE. Increased vertebral bone mineral in response to reduced exercise in amenorrheic runners. West J Med. 1987;146(1):39–42.
Cialdella-Kam L, Guebels CP, Maddalozzo GF, Manore MM. Dietary intervention restored menses in female athletes with exercise-associated menstrual dysfunction with limited impact on bone and muscle health. Nutrients. 2014;6(8):3018–39. doi:10.3390/nu6083018.
Arends JC, Cheung MY, Barrack MT, Nattiv A. Restoration of menses with nonpharmacologic therapy in college athletes with menstrual disturbances: a 5-year retrospective study. Int J Sport Nutr Exerc Metab. 2012;22(2):98–108.
Arimura C, Nozaki T, Takakura S, Kawai K, Takii M, Sudo N, et al. Predictors of menstrual resumption by patients with anorexia nervosa. Eat Weight Disord. 2010;15(4):e226–33. doi:10.3275/7039.
Cominato L, da Silva MM, Steinmetz L, Pinzon V, Fleitlich-Bilyk B, Damiani D. Menstrual cycle recovery in patients with anorexia nervosa: the importance of insulin-like growth factor 1. Horm Res Paediatr. 2014;82(5):319–23. doi:10.1159/000367895.
Dempfle A, Herpertz-Dahlmann B, Timmesfeld N, Schwarte R, Egberts KM, Pfeiffer E, et al. Predictors of the resumption of menses in adolescent anorexia nervosa. BMC Psychiatry. 2013;13:308. doi:10.1186/1471-244X-13-308.
El Ghoch M, Calugi S, Chignola E, Bazzani PV, Dalle Grave R. Body fat and menstrual resumption in adult females with anorexia nervosa: a 1-year longitudinal study. J Hum Nutr Diet. 2016;29(5):662–6. doi:10.1111/jhn.12373.
Golden NH, Jacobson MS, Schebendach J, Solanto MV, Hertz SM, Shenker IR. Resumption of menses in anorexia nervosa. Arch Pediatr Adolesc Med. 1997;151(1):16–21.
Misra M, Prabhakaran R, Miller KK, Goldstein MA, Mickley D, Clauss L, et al. Weight gain and restoration of menses as predictors of bone mineral density change in adolescent girls with anorexia nervosa-1. J Clin Endocrinol Metab. 2008;93(4):1231–7. doi:10.1210/jc.2007-1434.
Pitts S, Blood E, Divasta A, Gordon CM. Percentage body fat by dual-energy X-ray absorptiometry is associated with menstrual recovery in adolescents with anorexia nervosa. J Adolesc Health. 2014;54(6):739–41. doi:10.1016/j.jadohealth.2013.12.033.
van Elburg AA, Eijkemans MJ, Kas MJ, Themmen AP, de Jong FH, van Engeland H, et al. Predictors of recovery of ovarian function during weight gain in anorexia nervosa. Fertil Steril. 2007;87(4):902–8. doi:10.1016/j.fertnstert.2006.11.004.
• Gordon CM, Ackerman KE, Berga SL, Kaplan JR, Mastorakos G, Misra M, et al. Functional hypothalamic amenorrhea: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2017; doi:10.1210/jc.2017-00131. These evidence-based clinical practice guidelines were recently published by the Endocrine Society and comprehensively summarize the current recommendations for the evaluation, diagnosis, and treatment of functional hypothalamic amenorrhea.
Falsetti L, Gambera A, Barbetti L, Specchia C. Long-term follow-up of functional hypothalamic amenorrhea and prognostic factors. J Clin Endocrinol Metab. 2002;87(2):500–5. doi:10.1210/jcem.87.2.8195.
Faust JP, Goldschmidt AB, Anderson KE, Glunz C, Brown M, Loeb KL, et al. Resumption of menses in anorexia nervosa during a course of family-based treatment. J Eat Disord. 2013;1:12. doi:10.1186/2050-2974-1-12.
Abbate Daga G, Campisi S, Marzola E, Rocca G, Peris C, Campagnoli C, et al. Amenorrhea in eating disorders: poor stability of symptom after a one-year treatment. Eat Weight Disord. 2012;17(2):e78–85. doi:10.3275/7962.
Dei M, Seravalli V, Bruni V, Balzi D, Pasqua A. Predictors of recovery of ovarian function after weight gain in subjects with amenorrhea related to restrictive eating disorders. Gynecol Endocrinol. 2008;24(8):459–64. doi:10.1080/09513590802246141.
Favaro A, Santonastaso P. Seasonality and the prediction of weight at resumption of menses in anorexia nervosa. Fertil Steril. 2009;91(4 Suppl):1395–7. doi:10.1016/j.fertnstert.2008.04.055.
Rigaud D, Pennacchio H, Bizeul C, Reveillard V, Verges B. Outcome in AN adult patients: a 13-year follow-up in 484 patients. Diabetes Metab. 2011;37(4):305–11. doi:10.1016/j.diabet.2010.11.020.
Drinkwater BL, Nilson K, Ott S, Chesnut CH 3rd. Bone mineral density after resumption of menses in amenorrheic athletes. JAMA. 1986;256(3):380–2.
Warren MP, Brooks-Gunn J, Fox RP, Holderness CC, Hyle EP, Hamilton WG. Osteopenia in exercise-associated amenorrhea using ballet dancers as a model: a longitudinal study. J Clin Endocrinol Metab. 2002;87(7):3162–8. doi:10.1210/jcem.87.7.8637.
Baim S, Wilson CR, Lewiecki EM, Luckey MM, Downs RW Jr, Lentle BC. Precision assessment and radiation safety for dual-energy X-ray absorptiometry: position paper of the International Society for Clinical Densitometry. J Clin Densitom. 2005;8(4):371–8.
Allaway HC, Williams NI, Mallinson RJ, Koehler K, De Souza MJ. Reductions in urinary collection frequency for assessment of reproductive hormones provide physiologically representative exposure and mean concentrations when compared with daily collection. Am J Hum Biol. 2015;27(3):358–71. doi:10.1002/ajhb.22649.
Ross AC. The 2011 report on dietary reference intakes for calcium and vitamin D. Public Health Nutr. 2011;14(5):938–9. doi:10.1017/S1368980011000565.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–30. doi:10.1210/jc.2011-0385.
Winters-Stone KM, Snow CM. One year of oral calcium supplementation maintains cortical bone density in young adult female distance runners. Int J Sport Nutr Exerc Metab. 2004;14(1):7–17.
Gibson JH, Mitchell A, Reeve J, Harries MG. Treatment of reduced bone mineral density in athletic amenorrhea: a pilot study. Osteoporos Int. 1999;10(4):284–9. doi:10.1007/s001980050228.
Lappe J, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin d supplementation decreases incidence of stress fractures in female navy recruits. J Bone Miner Res. 2008;23(5):741–9. doi:10.1359/jbmr.080102.
Allaway HCM, Weaver CM, Petkus DL, Stone MS, Misra M, Martin M, et al. Oral and non-oral contraceptives decrease recombinant human GH-stimulated hepatic IGF-1 secretion in young women following two months of use. Orlando: ENDO; 2017.
Misra M, Katzman D, Miller KK, Mendes N, Snelgrove D, Russell M, et al. Physiologic estrogen replacement increases bone density in adolescent girls with anorexia nervosa. J Bone Miner Res. 2011;26(10):2430–8. doi:10.1002/jbmr.447.
Zofkova I. Pathophysiological and clinical importance of insulin-like growth factor-I with respect to bone metabolism. Physiol Res. 2003;52(6):657–79.
Crane JL, Cao X. Function of matrix IGF-1 in coupling bone resorption and formation. J Mol Med (Berl). 2014;92(2):107–15. doi:10.1007/s00109-013-1084-3.
Adami S, Zivelonghi A, Braga V, Fracassi E, Gatti D, Rossini M, et al. Insulin-like growth factor-1 is associated with bone formation markers, PTH and bone mineral density in healthy premenopausal women. Bone. 2010;46(1):244–7. doi:10.1016/j.bone.2009.10.011.
Giustina A, Mazziotti G, Canalis E. Growth hormone, insulin-like growth factors, and the skeleton. Endocr Rev. 2008;29(5):535–59. doi:10.1210/er.2007-0036.
Savage MO. Insulin-like growth factors, nutrition and growth. World Rev Nutr Diet. 2013;106:52–9. doi:10.1159/000342577.
Laughlin GA, Yen SS. Nutritional and endocrine-metabolic aberrations in amenorrheic athletes. J Clin Endocrinol Metab. 1996;81(12):4301–9. doi:10.1210/jcem.81.12.8954031.
Allaway HC, Southmayd EA, De Souza MJ. The physiology of functional hypothalamic amenorrhea associated with energy deficiency in exercising women and in women with anorexia nervosa. Horm Mol Biol Clin Investig. 2016;25(2):91–119. doi:10.1515/hmbci-2015-0053.
Christo K, Prabhakaran R, Lamparello B, Cord J, Miller KK, Goldstein MA, et al. Bone metabolism in adolescent athletes with amenorrhea, athletes with eumenorrhea, and control subjects. Pediatrics. 2008;121(6):1127–36. doi:10.1542/peds.2007-2392.
Genazzani AD, Petraglia F, Gastaldi M, Gamba O, Corazza F, D’Ambrogio G, et al. Growth hormone (GH)-releasing hormone-induced GH response in hypothalamic amenorrhea: evidence of altered central neuromodulation. Fertil Steril. 1996;65(5):935–8.
Russell M, Stark J, Nayak S, Miller KK, Herzog DB, Klibanski A, et al. Peptide YY in adolescent athletes with amenorrhea, eumenorrheic athletes and non-athletic controls. Bone. 2009;45(1):104–9. doi:10.1016/j.bone.2009.03.668.
Zanker CL, Swaine IL. The relationship between serum oestradiol concentration and energy balance in young women distance runners. Int J Sports Med. 1998;19(2):104–8. doi:10.1055/s-2007-971890.
Grinspoon SK, Baum HB, Peterson S, Klibanski A. Effects of rhIGF-I administration on bone turnover during short-term fasting. J Clin Invest. 1995;96(2):900–6. doi:10.1172/JCI118137.
Grinspoon S, Baum H, Lee K, Anderson E, Herzog D, Klibanski A. Effects of short-term recombinant human insulin-like growth factor I administration on bone turnover in osteopenic women with anorexia nervosa. J Clin Endocrinol Metab. 1996;81(11):3864–70. doi:10.1210/jcem.81.11.8923830.
Misra M, McGrane J, Miller KK, Goldstein MA, Ebrahimi S, Weigel T, et al. Effects of rhIGF-1 administration on surrogate markers of bone turnover in adolescents with anorexia nervosa. Bone. 2009;45(3):493–8. doi:10.1016/j.bone.2009.06.002.
Grinspoon S, Thomas L, Miller K, Herzog D, Klibanski A. Effects of recombinant human IGF-I and oral contraceptive administration on bone density in anorexia nervosa. J Clin Endocrinol Metab. 2002;87(6):2883–91. doi:10.1210/jcem.87.6.8574.
Ahima RS, Prabakaran D, Mantzoros C, Qu D, Lowell B, Maratos-Flier E, et al. Role of leptin in the neuroendocrine response to fasting. Nature. 1996;382(6588):250–2. doi:10.1038/382250a0.
Schwartz MW, Woods SC, Porte D Jr, Seeley RJ, Baskin DG. Central nervous system control of food intake. Nature. 2000;404(6778):661–71. doi:10.1038/35007534.
Miller KK, Parulekar MS, Schoenfeld E, Anderson E, Hubbard J, Klibanski A, et al. Decreased leptin levels in normal weight women with hypothalamic amenorrhea: the effects of body composition and nutritional intake. J Clin Endocrinol Metab. 1998;83(7):2309–12. doi:10.1210/jcem.83.7.4975.
Tataranni PA, Monroe MB, Dueck CA, Traub SA, Nicolson M, Manore MM, et al. Adiposity, plasma leptin concentration and reproductive function in active and sedentary females. Int J Obes Relat Metab Disord. 1997;21(9):818–21.
Kopp W, Blum WF, von Prittwitz S, Ziegler A, Lubbert H, Emons G, et al. Low leptin levels predict amenorrhea in underweight and eating disordered females. Mol Psychiatry. 1997;2(4):335–40.
Warren MP, Voussoughian F, Geer EB, Hyle EP, Adberg CL, Ramos RH. Functional hypothalamic amenorrhea: hypoleptinemia and disordered eating. J Clin Endocrinol Metab. 1999;84(3):873–7. doi:10.1210/jcem.84.3.5551.
Christo K, Cord J, Mendes N, Miller KK, Goldstein MA, Klibanski A, et al. Acylated ghrelin and leptin in adolescent athletes with amenorrhea, eumenorrheic athletes and controls: a cross-sectional study. Clin Endocrinol. 2008;69(4):628–33. doi:10.1111/j.1365-2265.2008.03237.x.
Ackerman KE, Slusarz K, Guereca G, Pierce L, Slattery M, Mendes N, et al. Higher ghrelin and lower leptin secretion are associated with lower LH secretion in young amenorrheic athletes compared with eumenorrheic athletes and controls. Am J Physiol Endocrinol Metab. 2012;302(7):E800–6. doi:10.1152/ajpendo.00598.2011.
Chan JL, Mantzoros CS. Role of leptin in energy-deprivation states: normal human physiology and clinical implications for hypothalamic amenorrhoea and anorexia nervosa. Lancet. 2005;366(9479):74–85. doi:10.1016/S0140-6736(05)66830-4.
Mantzoros CS, Magkos F, Brinkoetter M, Sienkiewicz E, Dardeno TA, Kim SY, et al. Leptin in human physiology and pathophysiology. Am J Physiol Endocrinol Metab. 2011;301(4):E567–84. doi:10.1152/ajpendo.00315.2011.
Welt CK, Chan JL, Bullen J, Murphy R, Smith P, DePaoli AM, et al. Recombinant human leptin in women with hypothalamic amenorrhea. N Engl J Med. 2004;351(10):987–97. doi:10.1056/NEJMoa040388.
Chou SH, Chamberland JP, Liu X, Matarese G, Gao C, Stefanakis R, et al. Leptin is an effective treatment for hypothalamic amenorrhea. Proc Natl Acad Sci U S A. 2011;108(16):6585–90. doi:10.1073/pnas.1015674108.
Sienkiewicz E, Magkos F, Aronis KN, Brinkoetter M, Chamberland JP, Chou S, et al. Long-term metreleptin treatment increases bone mineral density and content at the lumbar spine of lean hypoleptinemic women. Metabolism. 2011;60(9):1211–21. doi:10.1016/j.metabol.2011.05.016.
Holly J, Perks C. The role of insulin-like growth factor binding proteins. Neuroendocrinology. 2006;83(3–4):154–60. doi:10.1159/000095523.
Gatti R, De Palo EF, Antonelli G, Spinella P. IGF-I/IGFBP system: metabolism outline and physical exercise. J Endocrinol Investig. 2012;35(7):699–707. doi:10.3275/8456.
Karlsson R, Eden S, von Schoultz B. Altered growth hormone secretion during oral contraception. Gynecol Obstet Investig. 1990;30(4):234–8.
Balogh A, Kauf E, Vollanth R, Graser G, Klinger G, Oettel M. Effects of two oral contraceptives on plasma levels of insulin-like growth factor I (IGF-I) and growth hormone (hGH). Contraception. 2000;62(5):259–69.
Jernstrom H, Deal C, Wilkin F, Chu W, Tao Y, Majeed N, et al. Genetic and nongenetic factors associated with variation of plasma levels of insulin-like growth factor-I and insulin-like growth factor-binding protein-3 in healthy premenopausal women. Cancer Epidemiol Biomark Prev. 2001;10(4):377–84.
Jernstrom H, Olsson H. Suppression of plasma insulin-like growth factor-1 levels in healthy, nulliparous, young women using low dose oral contraceptives. Gynecol Obstet Investig. 1994;38(4):261–5.
Blackmore KM, Wong J, Knight JA. A cross-sectional study of different patterns of oral contraceptive use among premenopausal women and circulating IGF-1: implications for disease risk. BMC Womens Health. 2011;11:15. doi:10.1186/1472-6874-11-15.
Harel Z, Riggs S, Vaz R, Flanagan P, Harel D, Machan JT. Bone accretion in adolescents using the combined estrogen and progestin transdermal contraceptive method Ortho Evra: a pilot study. J Pediatr Adolesc Gynecol. 2010;23(1):23–31. doi:10.1016/j.jpag.2009.04.008.
• Southmayd EA, De Souza MJ. A summary of the influence of exogenous estrogen administration across the lifespan on the GH/IGF-1 axis and implications for bone health. Growth Hormon IGF Res. 2017;32:2–13. doi:10.1016/j.ghir.2016.09.001. This review summarizes our current understanding of the impact of exogenous estrogen administration on the GH/IGF-1 axis and bone health outcomes in pre- and post-menopausal women.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Emily Southmayd, Adelaide Hellmers, and Mary Jane De Souza declare no conflict of interest.
Human and Animal Rights and Informed Consent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Additional information
This article is part of the Topical Collection on Nutrition, Exercise, and Lifestyle in Osteoporosis
Rights and permissions
About this article

Cite this article
Southmayd, E.A., Hellmers, A.C. & De Souza, M.J. Food Versus Pharmacy: Assessment of Nutritional and Pharmacological Strategies to Improve Bone Health in Energy-Deficient Exercising Women. Curr Osteoporos Rep 15, 459–472 (2017). https://doi.org/10.1007/s11914-017-0393-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11914-017-0393-9