
Abstract
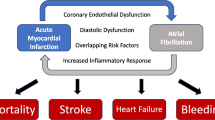
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and is a frequent complication of acute myocardial infarction (MI). AF occurs in 5% to 10% of patients who have received fibrinolysis. Post-MI AF is more common in older patients, in patients with heart failure, and after more extensive infarction. Postinfarction prognosis is worse among patients complicated by AF—indeed, mortality and morbid events including stroke, thromboembolism, and heart failure are increased in this group. It is unclear as to whether AF directly reduces survival or merely demarcates patients at higher overall risk. Despite its frequent occurrence and deleterious influence on outcomes, randomized data regarding management of AF after acute MI are scarce. This review summarizes recent data charting the incidence of AF after acute MI and describes features associated with its occurrence. Clinical sequelae and current principles in treatment are also discussed.
Similar content being viewed by others


References and Recommended Reading
Benjamin EJ, Levy D, Vaziri SM, et al.: Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA 1994, 271:840–844.
Kannel WB, Wolf PA, Benjamin EJ, Levy D: Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol 1998, 82:2N-9N.
Benjamin EJ, Wolf PA, D’Agostino RB, et al.: Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation 1998, 98:946–952.
Lin HJ, Wolf PA, Kelly-Hayes M, et al.: Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996, 27:1760–1764.
Wattigney WA, Mensah GA, Croft JB: Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: implications for primary prevention. Circulation 2003, 108:711–716.
Stewart S, Murphy N, Walker A, et al.: Cost of an emerging epidemic: an economic analysis of atrial fibrillation in the UK. Heart 2004, 90:286–292.
Crenshaw BS, Ward SR, Granger CB, et al.: Atrial fibrillation in the setting of acute myocardial infarction: the GUSTO-I experience. Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries. J Am Coll Cardiol 1997, 30:406–413.
Sakata K, Kurihara H, Iwamori K, et al.: Clinical and prognostic significance of atrial fibrillation in acute myocardial infarction. Am J Cardiol 1997, 80:1522–1527.
Eldar M, Canetti M, Rotstein Z, et al.: Significance of paroxysmal atrial fibrillation complicating acute myocardial infarction in the thrombolytic era. SPRINT and Thrombolytic Survey Groups. Circulation 1998, 97:965–970.
Pedersen OD, Bagger H, Kober L, Torp-Pedersen C: The occurrence and prognostic significance of atrial fibrillation/-flutter following acute myocardial infarction. TRACE Study group. TRAndolapril Cardiac Evaluation.Eur Heart J 1999, 20:748–754.
Carlsson J, Tebbe U, Neuhaus KL, et al. Atrial fibrillation in acute myocardial infarction: data from the inTIME-II study. Circulation 1999, 100(Suppl 1):abstract 2636.
Wong CK, White HD, Wilcox RG, et al.: New atrial fibrillation after acute myocardial infarction independently predicts death: the GUSTO-III experience. Am Heart J 2000, 140:878–885.
Rathore SS, Berger AK, Weinfurt KP, et al.: Acute myocardial infarction complicated by atrial fibrillation in the elderly: prevalence and outcomes. Circulation 2000, 101:969–974. This large survey of more than 100,000 health care beneficiaries noted that AF independently predicted mortality after AMI.
Pizzetti F, Turazza FM, Franzosi MG, et al.: Incidence and prognostic significance of atrial fibrillation in acute myocardial infarction: the GISSI-3 data. Heart 2001, 86:527–532.
Goldberg RJ, Yarzebski J, Lessard D, et al.: Recent trends in the incidence rates of and death rates from atrial fibrillation complicating initial acute myocardial infarction: a community-wide perspective. Am Heart J 2002, 143:519–527. This is an observational study conducted between 1990 and 1997. Incidence of AF after AMI decreased from 18% to 11% during this period. Survival for patients with AF tended to improve.
Mehta RH, Dabbous OH, Granger CB, et al.: Comparison of outcomes of patients with acute coronary syndromes with and without atrial fibrillation. Am J Cardiol 2003, 92:1031–1036.
Kinjo K, Sato H, Sato H, et al.: Prognostic significance of atrial fibrillation/atrial flutter in patients with acute myocardial infarction treated with percutaneous coronary intervention. Am J Cardiol 2003, 92:1150–1154.
Celik S, Erdol C, Baykan M, et al.: Relation between paroxysmal atrial fibrillation and left ventricular diastolic function in patients with acute myocardial infarction. Am J Cardiol 2001, 88:160–162, A5.
Rosiak M, Ruta J, Bolinska H: Usefulness of prolonged P-wave duration on signal averaged ECG predicting atrial fibrillation in acute myocardial infarction patients. Med Sci Monit 2003, 9:85–88.
Pedersen OD, Bagger H, Kober L, Torp-Pedersen C: Trandolapril reduces the incidence of atrial fibrillation after acute myocardial infarction in patients with left ventricular dysfunction. Circulation 1999, 100:376–380.
Shinbane JS, Wood MA, Jensen DN, et al.: Tachycardia-induced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol 1997, 29:709–715.
Lip GYH: Does atrial fibrillation confer a hypercoagulable state? Lancet 1995, 346:1313–1314.
Hohnloser SH, Kuck KH, Lilienthal J: Rhythm or rate control in atrial fibrillation--Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial. Lancet 2000, 356:1789–1794.
Van Gelder IC, Hagens VE, Bosker HA, et al.: A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med 2002, 347:1834–1840.
Wyse DG, Waldo AL, DiMarco JP, et al.: A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med 2002, 347:1825–1833. This is a large, randomized study reporting noninferiority of rate control compared with rhythm control in AF. Whether either strategy is superior in AMI requires evaluation.
ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation--executive summary.Eur Heart J 2001, 20:1852–1923.
Echt DS, Liebson PR, Mitchell LB, et al.: Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med 1991, 324:781–788.
Julian DG, Camm AJ, Frangin G, et al.: Randomised trial of effect of amiodarone on mortality in patients with leftventricular dysfunction after recent myocardial infarction: EMIAT. European Myocardial Infarct Amiodarone Trial Investigators. Lancet 1997, 349:667–674.
Cairns JA, Connolly SJ, Roberts R, Gent M: Randomised trial of outcome after myocardial infarction in patients with frequent or repetitive ventricular premature depolarisations: CAMIAT. Canadian Amiodarone Myocardial Infarction Arrhythmia Trial Investigators. Lancet 1997, 349:675–682.
Kilborn MJ, Rathore SS, Gersh BJ, et al.: Amiodarone and mortality among elderly patients with acute myocardial infarction with atrial fibrillation. Am Heart J 2002, 144:1095–1101.
Essebag V, Hadjis T, Platt RW, Pilote L: Amiodarone and the risk of bradyarrhythmia requiring permanent pacemaker in elderly patients with atrial fibrillation and prior myocardial infarction. J Am Coll Cardiol 2003, 41:249–254.
Kontoyannis DA, Anastasiou-Nana MI, Kontoyannis SA, et al.: Intravenous amiodarone decreases the duration of atrial fibrillation associated with acute myocardial infarction. Cardiovasc Drugs Ther 2001, 15:155–160.
Kober L, Bloch Thomsen PE, Moller M, et al.: Effect of dofetilide in patients with recent myocardial infarction and left-ventricular dysfunction: a randomised trial. Lancet 2000, 356:2052–2058. This paper reviews the use of dofetilide versus placebo in recent MI patients with ejection fraction less than 35%. Dofetilide did not increase mortality and appeared effective in cardioverting AF in the subgroup.
Wong CK, White HD, Wilcox RG, et al.: Management and outcome of patients with atrial fibrillation during acute myocardial infarction: the GUSTO-III experience. Global Use of Strategies to Open Occluded Coronary Arteries. Heart 2002, 88:357–362. In this observational substudy, class I antiarrhythmic and sotalol treatment associated a with trend toward better survival, but not improved cardioversion.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bhatia, G.S., Lip, G.Y.H. Atrial fibrillation post-myocardial infarction: Frequency, consequences, and management. Curr Heart Fail Rep 1, 149–155 (2004). https://doi.org/10.1007/s11897-004-0002-y
Issue Date:
DOI: https://doi.org/10.1007/s11897-004-0002-y