
Abstract
Purpose of Review
Cardiovascular and endothelial dysfunction is recognized nowadays as an important etiological factor contributing to the development of hypertensive disorders of pregnancy.
Recent Findings
Preeclampsia is considered a specific disease of pregnancy, but recent theories suggest that women suffering from the condition have greater propensity to develop atherosclerosis, heart disease, and stroke over the years.
Summary
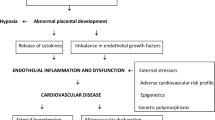
It is possible that transient but severe endothelial dysfunction observed in preeclampsia potentiates a cascade of events that progresses to atherosclerosis. Preeclampsia offers a unique window of opportunity to identify maternal endothelial dysfunction and pre-existing cardiovascular disease. The placenta is closely involved in the onset of preeclampsia, but endothelial and cardiac vascular factors also play important causal roles in the development of hypertension during pregnancy. According to the data presented, it is clear that preeclampsia selects a group at high risk of development of atherosclerosis and at increased cardiovascular risk, as well as of stroke, in the decades following childbirth.
Similar content being viewed by others


References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Bell MJ. A historical overview of preeclampsia-eclampsia. J Obstet Gynecol Neonatal Nurs. 2010 September;39(5):510–8.
Ong S. Pre-eclampsia: a historical perspective. In: Baker PN, Kingdom JCP, editors. Pre-eclampsia: current perspectives on management. New York: The Parthenon Publishing Group; 2004. p. 15–24.
Hidaka A, Nakamoto O. Historical perspective of preeclampsia from the viewpoint of pathogenesis: ancient times to mid-20th century. Hypertens Res Pregnancy. 2014;2:40–6.
Maynard SE, Min JY, Merchan J, et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003;111(05):649–58.
Roberts JM, Hubel CA. The two stage model of preeclampsia: variations on the theme. Placenta. 2009;30(Suppl A):S32–7. https://doi.org/10.1016/j.placenta.2008.11.009.
Quinn MJ. Pre-eclampsia - The “uterine reinnervation” view. Med Hypotheses. 2014;83(05):575–9.
Abou El Hassan M, Diamandis EP, Karumanchi SA, Shennan AH, Taylor RN. Preeclampsia: an old disease with new tools for better diagnosis and risk management. Clin Chem. 2015;61(05):694–8.
Tanrikulu L, Naraghi R, Ernst V, et al. Neurovascular compression of medulla oblongata - association for gestation-induced hypertension. Med Hypotheses. 2015;84:605–10.
Gathiram P, Moodley J. Pre-eclampsia: its pathogenesis and pathophysiolgy. Cardiovasc J Afr. 2016;27(02):71–8.
Brew O, Sullivan MHF, Woodman A. Comparison of normal and pre-eclamptic placental gene expression: a systematic review with meta-analysis. PLoS One. 2016 Aug 25;11(08):e0161504. https://doi.org/10.1371/journal.pone.0161504. eCollection 2016.
Cunningham GF, Leveno KJ, Bloom SL, et al. Williams Obstetrics. 24th ed. New York: McGraw-Hill Education; 2014.
Ngene NC, Moodley J. Role of angiogenic factors in the pathogenesis and management of pre-eclampsia. Int J Gynaecol Obstet. 2018;41(01):5–13.
Kim J-Y, Kim YM. Acute Atherosis of the uterine spiral arteries: Clinicopathologic implications. J Pathol Transl Med; 2015;49:462–71.
Muijsers HEC, Roeleveld N, van der Heijden OWH, Maas AHEM. Consider preeclampsia as a first cardiovascular event. Curr Cardiovasc Risk Rep. 2019;13:21.
Bellamy L, Casas J-P, Hingorani AD, Williams DJ. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. 2007:335–974.
•• Kalafat E, Thilaganathan B. Cardiovascular origins of preeclampsia. Curr Opin Obstet Gynecol. 2017;29(6):383–9. Considering preeclampsia to be a cardiovascular syndrome.
Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365(9461):785–99.
Ventura SJ, Menacker CS, Births F. final data for 1999. In: National Vital Statistics Report, vol. 49; 2001.
Silva JMP, Fonseca SC, Dias MAB, Izzo AS, Teixeira GP, Belfort PP. Concepts, prevalence and characteristics of severe maternal morbidity and near miss in Brazil: a systematic review. Rev Bras Saude Mater Infant; 2018;18(1).
Ramos JGL, Sass N, Costa SHM. Preeclampsia. Rev Bras Ginecol Obstet. 2017;39:496–512.
Behrens I, Basit S, Melbye M, Lykke JA, Wohlfahrt J, Bundgaard H, et al. Risk of post-pregnancy hypertension in women with a history of hypertensive disorders of pregnancy: nationwide cohort study. BMJ. 2017;358:j3078.
Grand’Maison S, Pilote L, Schlosser K, Stewart DJ, Okano M, Dayan N. Clinical features and outcomes of acute coronary syndrome in women with previous pregnancy complications. Can J Cardiol. 2017;33:1683–92.
American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists' Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122(05):1122–31.
Brown MA, Magee LA, Kenny LC, et al. International Society for the Study of hypertension in pregnancy (ISSHP). Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72(01):24–43.
Peraçoli JC, Borges VTM, et al. Pre-eclampsia/Eclampsia. Rev Bras Ginecol Obstet. 2019;41(5):318–32.
von Dadelzen P, Payne B, Li J, et al. Prediction of adverse maternal outcomes in preeclampsia: development and validation of the fullPIERS model. Lancet. 2011;377:219–27.
Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005;308:1592–4.
Romero R, Chaiworapongsa T. Preeclampsia: a link between trophoblast dysregulation and an antiangiogenic state. J Clin Invest. 2013;123:2775–7.
Rana S, Lemoine E, Granger J, Karumanchi AS. Preeclampsia. Pathophysiology, challenges, and perspectives. Circ Res. 2019;124:1094–112.
Herraiz I, Llurba E, Verlohren S, Galindo A. Update on the diagnosis and prognosis of preeclampsia with the aid of the sFlt-1/ PlGF ratio in singleton pregnancies. Fetal Diagn Ther. 2018;43(2):81–9.
Valensise H, Vasapollo B, Gagliardi G, Novelli GP. Early and late preeclampsia: two different maternal hemodynamic states in the latent phase of the disease. Hypertension. 2008 Nov;52(5):873–80.
Castleman JS, Ganapathy R, Taki F, Lip GY, Steeds RP, Kotecha D. Echocardiographic structure and function in hypertensive disorders of pregnancy: a systematic review. Circ Cardiovasc Imaging. 2016;9(9).
•• Melchiorre K, Sharma R, Thilaganathan B. Maternal cardiovascular function in normal pregnancy: evidence of maladaptationormal to chronic volume overload. Hypertension. 2016;67:754–62. Longitudinal study that demonstraded cardiac dysfunction in a small but significant group of women at term.
Timokhina E, Kuzmina T, Strizhakov A, Pitskhelauri E, Ignatko I, Belousova V. Maternal cardiac function after normal delivery, preeclampsia, and eclampsia: a prospective study. J Pregnancy. 2019;2019:8.
Simmons LA, Gillin AG, Jeremy RW. Structural and functional changes in left ventricle during normotensive and preeclamptic pregnancy. Am J Physiol Heart Circ Physiol. 2002 Oct;283(4):H1627–33.
Alves Borges JH, Goes DA, de Araújo LB, Dos Santos MC, Debs Diniz AL. Prospective study of the hemodynamic behavior of ophthalmic arteries in postpartum preeclamptic women: a doppler evaluation. Hypertens Pregnancy. 2016;35(1):100–11.
Diniz AL, Moron AF, dos Santos MC, Sass N, Pires CR, Debs CL. Ophthalmic artery Doppler as a measure of severe pre-eclampsia. Int J Gynaecol Obstet. 2008 Mar;100(3):216–20.
Maruyoshi H, Kojima S, Kojima S, Nagayoshi Y, Horibata Y, Kaikita K, et al. Waveform of ophthalmic artery Doppler flow predicts the severity of systemic atherosclerosis. Circ J. 2010 Jun;74(6):1251–6.
Koelwyn, Graeme & Currie, Katharine & Macdonald, Maureen & Eves, Neil. (2012). Ultrasonography and tonometry for the assessment of human arterial stiffness. https://doi.org/10.5772/39193. Available from: https://www.intechopen.com/books/applied-aspects-of-ultrasonography-in-humans/ultrasonography-and-tonometry-for-the-assessment-of-human-arterial-stiffness.
Roberts JM, Gammill HS. Preeclampsia: recent insights. Hypertension. 2005;46(6).
Amaral LM, Cunningham MW Jr, Cornelius DC, LaMarca B. Preeclampsia: long-term consequences for vascular health. Vasc Health Risk Manag. 2015;15:11–4.
Çintesun E, Incesu Çintesun FN, Ezveci H, Akyürek F, Çelik Ç. Systemic inflammatory response markers in preeclampsia. J Lab & Physicians. 2018;10(3):316–9.
Pant V, Yadav BK, Sharma J. A cross sectional study to assess the sFlt-1:PlGF ratio in pregnant women with and without preeclampsia. BMC Pregnancy Childbirth. 2019;19(1):266.
Arun Jeyabalan A, Powers RW, Durica AR, Harger G, Roberts JM, Ness RB. Cigarette smoke exposure and angiogenic factors in pregnancy and preeclampsia. Am J Hypertens. 2008;21(8):943–7.
Paes MMBM, Diniz ALD. Chronic perfusion changes and reduction in preeclampsia incidence in pregnant smokers: an ophthalmic artery Doppler study. J Matern Fetalx Neonatal Med. 2015;28(17):2074–9.
Bellamy L, Casas J-P, Hingorani AD, Williams DJ. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. 2007;335:974.
Rangaswami J, Naranjo M, McCullough PA. Preeclampsia as a form of type 5 cardiorenal syndrome: an underrecognized entity in women’s cardiovascular health. Cardiorenal Med. 2018;8(2):160–72.
Kessous R, Shoham-Vardi I, Pariente G, Sergienko R, Sheiner E. Long-term maternal atherosclerotic morbidity in women with pre-eclampsia. Heart. 2015;101(6):442–6.
Christensen M, Kronborg CS, Carlsen RK, et al. Early gestational age at preeclampsia onset is associated with subclinical atherosclerosis 12 years after delivery. Acta Obstet Gynecol Scand. 2017 Sep;96(9):1084–92.
• Milic NM, Milin-Lazovic J, Weissgerber TL, Trajkovic G, White WM, Garovic VD. Preclinical atherosclerosis at the time of preeclamptic pregnancy and up to 10 years postpartum: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2017;49(1):110–5. Atherosclerotic load is present at the time of preeclampsia and may be one mechanism associated with preeclampsia.
Crandon AJ, Isherwood DM. Effect of aspirin on incidence of pre-eclampsia. Lancet. 1979;1:1356.
Rolnik DL, Wright D, Poon LC, O'Gorman N, Syngelaki A, de Paco Matallana C, et al. Aspirin versus placebo in pregnancies at high risk for preterm preeclampsia. N Engl J Med. 2017;377(7):613–22.
Roberge S, Bujold E, Nicolaides KH. Aspirin for the prevention of preterm and term preeclampsia: systematic review and metaanalysis. Am J Obstet Gynecol. 2018;218(3):287–93.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Angélica Lemos Debs Diniz, Maria Marta Bini Martins Paes, and Aline Debs Diniz each declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
All reported studies/experiments with human or animal subjects performed by the authors have been previously published and complied with all applicable ethical standards (including the Helsinki Declaration and its amendments, institutional/national research committee standards, and international/national/institutional guidelines).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Evidence-Based Medicine, Clinical Trials and Their Interpretations
Rights and permissions
About this article

Cite this article
Diniz, A.L.D., Paes, M.M.B.M. & Diniz, A.D. Analyzing Preeclampsia as the Tip of the Iceberg Represented by Women with Long-Term Cardiovascular Disease, Atherosclerosis, and Inflammation. Curr Atheroscler Rep 22, 13 (2020). https://doi.org/10.1007/s11883-020-0830-6
Published:
DOI: https://doi.org/10.1007/s11883-020-0830-6