
Abstract
Red yeast rice is an ancient Chinese dietary staple and medication used by millions of patients as an alternative therapy for hypercholesterolemia. In recent years, the use of red yeast rice has grown exponentially due to increased public interest in complementary and alternative medications and the publication of several randomized, controlled trials demonstrating its efficacy and safety in different populations. The most promising role for red yeast rice is as an alternative lipid-lowering therapy for patients who refuse to take statins because of philosophical reasons or patients who are unable to tolerate statin therapy due to statin-associated myalgias. However, there is limited government oversight of red yeast rice products, wide variability of active ingredients in available formulations, and the potential of toxic byproducts. Therefore, until red yeast rice products are regulated and standardized, physicians and patients should be cautious in recommending this promising alternative therapy for hyperlipidemia.

Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance ••Of major importance
Ma J, Li Y, Li J, et al. Constituents of Red Yeast Rice, a Traditional Chinese Food and Medicine. J. Agric Food Chem. 2000;48:5220–5225.
Van Tieghem P. Monascus, genre nouveau de l’ordre des Ascomycetes. Bull Soc France. 1884;31:226–231.
Went FA. Monascus purpureus le chmpignon de l’angquac une nouvelle thelobolee. Ann Soc Nat Bot. 1895;8:1–17.
•• Becker DJ, Gordon RY, Halbert SC, French B, Morris PB, Rader DJ. Red yeast rice for dyslipidemia in statin-intolerant patients: a randomized trial. Ann Intern Med. 2009;150(12):830–9, W147-9. This is the first trial evaluating red yeast rice as a lipid-lowering therapy for patients with a history of SAMs. It randomized 62 patients with a history of intolerance to one or more statins to a lifestyle-modification program and either red yeast rice or placebo and followed them for 24 weeks. The red yeast rice group had a significant decrease in LDL-C compared with placebo at 12 and 24 weeks, with no increase incidence in myalgias.
•• Becker DJ, Gordon RY, Morris PB, et al. Simvastatin vs therapeutic lifestyle changes and supplements: randomized primary prevention trial. Mayo Clin Proc. 2008;83(7):758–64. This trial that randomized 74 patients to either usual therapy (simvastatin) or an alternative regimen (red yeast rice, fish oil, and a lifestyle-modification program) and followed them for 12 weeks. There were no differences between the groups in LDL-C levels and the alternative-regimen group had significant decreases in weight and triglycerides.
Bogsrud MP, Ose L, Langslet G, et al. HypoCol (red yeast rice) lowers plasma cholesterol—a randomized placebo controlled study. Scand Cardiovasc J;44(4):197–200.
• Halbert SC, French B, Gordon RY, et al.: Tolerability of red yeast rice (2,400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previous statin intolerance. Am J Cardiol 2010, 105:198–204. This is the second trial evaluating red yeast rice as an alternative lipid-lowering therapy for patients with a history of SAMs. It randomized 43 patients to red yeast rice or pravastatin and followed them for 12 weeks. There were no differences between groups in the incidence of myalgias, muscle strength, or LDL-C lowering. There was a trend toward decreased myalgias in the red yeast rice group.
Lu Z, Kou W, Du B, et al. Effect of Xuezhikang, an extract from red yeast Chinese rice, on coronary events in a Chinese population with previous myocardial infarction. Am J Cardiol. 2008;101(12):1689–93.
Venero CV, Venero JV, Wortham DC, Thompson PD. Lipid-lowering efficacy of red yeast rice in a population intolerant to statins. Am J Cardiol. 2010;105(5):664–6.
McGowan MP, Proulx S. Nutritional supplements and serum lipids: does anything work? Curr Atheroscler Rep. 2009;11(6):470–6.
Li YG, Zhang F, Wang ZT, Hu ZB. Identification and chemical profiling of monacolins in red yeast rice using high-performance liquid chromatography with photodiode array detector and mass spectrometry. J Pharm Biomed Anal. 2004;35(5):1101–12.
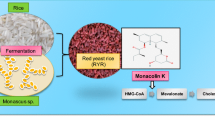
Endo A. Monacolin K, a new hypocholesterolemic agent produced by a Monascus species. J Antiobiot (Tokyo). 1979;32(8):852–4.
Gordon RY, Obermeyer W, Cooperman T, Becker DJ. Marked variability of monacolin levels in commercial red yeast rice products. Arch Intern Med. 2010;170(19):1722–27.
Heber D, Yip I, Ashley JM, Elashoff DA, Elashoff RM, Go VL. Cholesterol-lowering effects of a proprietary Chinese red-yeast-rice dietary supplement. Am J Clin Nutr. 1999;69(2):231–6.
Huang CF, Li TC, Lin CC, Liu CS, Shih HC, Lai MM. Efficacy of Monascus purpureus Went rice on lowering lipid ratios in hypercholesterolemic patients. Eur J Cardiovasc Prev Rehabil. 2007;14(3):438–40.
Liu J, Zhang J, Shi Y, Grimsgaard S, Alraek T, Fonnebo V. Chinese red yeast rice (Monascus purpureus) for primary hyperlipidemia: a meta-analysis of randomized controlled trials. Chin Med. 2006;1:4.
•• Li JJ, Lu ZL, Kou WR, et al. Beneficial Impact of Xuezhikang on Cardiovascular Events and Mortality in Elderly Hypertensive Patients With Previous Myocardial Infarction From the China Coronary Secondary Prevention Study (CCSPS). J Clin Pharmacol. 2009;49(8):947–956. This is the only trial that demonstrated that red yeast rice decreases cardiovascular events. Nearly 4870 Chinese patients with a history of myocardial infarction were randomized to red yeast rice or placebo and followed for 4.5 years. The red yeast group had significant decreases in overall mortality, cardiovascular mortality, and cardiovascular events compared with placebo.
Zhao SP, Lu ZL, Du BM, et al. Xuezhikang, an extract of cholestin, reduces cardiovascular events in type 2 diabetes patients with coronary heart disease: subgroup analysis of patients with type 2 diabetes from China coronary secondary prevention study (CCSPS). J Cardiovasc Pharmacol. 2007;49(2):81–4.
Jacobson TA. Toward “pain-free” statin prescribing: clinical algorithm for diagnosis and management of myalgia. Mayo Clin Proc. 2008;83(6):687–700.
Vandenberg BF, Robinson J. Management of the patient with statin intolerance. Curr Atheroscler Rep. 2010;12(1):48–57.
Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. Jama. 2003;289(13):1681–90.
Kashani A, Phillips CO, Foody JM, et al. Risks associated with statin therapy: a systematic overview of randomized clinical trials. Circulation. 2006;114(25):2788–97.
Mitka M. Expanding statin use to help more at-risk patients is causing financial heartburn. Jama. 2003;290(17):2243–5.
Hansen KE, Hildebrand JP, Ferguson EE, Stein JH. Outcomes in 45 patients with statin-associated myopathy. Arch Intern Med. 2005;165(22):2671–6.
Cartin-Ceba R, Lu LB, Kolpakchi A. A ‘natural’ threat. Am J Med. 2007;120(11):e3–4.
Mueller PS. Symptomatic myopathy due to red yeast rice. Ann Intern Med. 2006;145(6):474–5.
Smith DJ, Olive KE. Chinese red rice-induced myopathy. South Med J. 2003;96(12):1265–7.
Vercelli L, Mongini T, Olivero N, Rodolico C, Musumeci O, Palmucci L. Chinese red rice depletes muscle coenzyme Q10 and maintains muscle damage after discontinuation of statin treatment. J Am Geriatr Soc. 2006;54(4):718–20.
Lapi F, Gallo E, Bernasconi S, et al. Myopathies associated with red yeast rice and liquorice: spontaneous reports from the Italian Surveillance System of Natural Health Products. Br J Clin Pharmacol. 2008.
Roselle H, Ekatan A, Tzeng J, Sapienza M, Kocher J. Symptomatic hepatitis associated with the use of herbal red yeast rice. Ann Intern Med. 2008;149(7):516–7.
Wigger-Alberti W, Bauer A, Hipler UC, Elsner P. Anaphylaxis due to Monascus purpureus-fermented rice (red yeast rice). Allergy. 1999;54(12):1330–1.
Heber D, Lembertas A, Lu QY, Bowerman S, Go VL. An analysis of nine proprietary Chinese red yeast rice dietary supplements: implications of variability in chemical profile and contents. J Altern Complement Med. 2001;7(2):133–9.
Weiss R. Tainted Chinese Exports Common. Washington Post. May 20, 2007;http://www.washingtonpost.com/wp-dyn/content/article/2007/05/19/AR2007051901273.html. Accessed September 17, 2010.
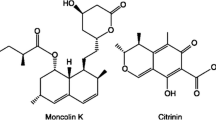
Endo A, Kuroda M. Citrinin, an inhibitor of cholesterol synthesis. J Antibiot (Tokyo). 1976;29(8):841–3.
Bennett JW, Klich M. Mycotoxins. Clin Microbiol Rev. 2003;16(3):497–516.
Havel RJ. Dietary supplement or drug? The case of cholestin. Am J Clin Nutr. 1999;69(2):175–6.
Miller SJ. Letter to Dirk Reischig, Nature’s Way Products, Inc. January 25, 2008. http://www.fda.gov/ICECI/EnforcementActions/WarningLetters/2008/ucm1048419.htm. Accessed September 18, 2010.
Kimpel P. The Cholestin Case: Drugs vs. Supplements. http://iml.jou.ufl.edu/projects/Spring2000/Kimpel/cholestin.html. Accessed September 18, 2010.
Moore RJ. Letter to Sonia Rodriguez, Mason Vitamins. May 5, 2001. http://www.fda.gov/OHRMS/DOCKETS/dailys/01/Jun01/061101/let0494.pdf. Accessed September 18, 2010.
Lee T. Ask the doctor. What is the story on using red yeast rice to lower cholesterol? You have warned readers against using it in the past, but I heard about a new study that shows it works. Are you ready to admit you are wrong on this one? Harv Heart Lett. 2009;20(4):8.
Phillips PS. Balancing randomized trials with anecdote. Ann Intern Med. 2009;150(12):885–6.
Carter M, O’Keefe JH, Becker DJ, Gordon RY, Gordon J. Is red yeast rice a suitable alternative for statins? Mayo Clin Proc. 2008;83(11):1294; author reply 1294–6.
Joy TR, Hegele RA. Narrative review: statin-related myopathy. Ann Intern Med. 2009;150(12):858–68.
Stengler MA. Are Statin Drugs Destroying Your Muscles? http://www.bottomlinesecrets.com/article.html?article_id=100000937. 2010:Accessed September 13, 2010.
Brown BG, Zhao XQ, Chait A, et al. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med. 2001;345(22):1583–92.
Durrington PN, Bhatnagar D, Mackness MI, et al. An omega-3 polyunsaturated fatty acid concentrate administered for one year decreased triglycerides in simvastatin treated patients with coronary heart disease and persisting hypertriglyceridaemia. Heart. 2001;85(5):544–8.
Goldberg AC, Ostlund RE, Jr., Bateman JH, Schimmoeller L, McPherson TB, Spilburg CA. Effect of plant stanol tablets on low-density lipoprotein cholesterol lowering in patients on statin drugs. Am J Cardiol. 2006;97(3):376–9.
Siddiqi SA, Thompson PD. How do you treat patients with myalgia who take statins? Curr Atheroscler Rep. 2009;11(1):9–14.
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). Jama. 2001;285(19):2486–97
Marcoff L, Thompson PD. The role of coenzyme Q10 in statin-associated myopathy: a systematic review. J Am Coll Cardiol. 2007;49(23):2231–7.
Lee JH, O’Keefe JH, Bell D, Hensrud DD, Holick MF. Vitamin D deficiency an important, common, and easily treatable cardiovascular risk factor? J Am Coll Cardiol. 2008;52(24):1949–56.
Moreyra AE, Wilson AC, Koraym A. Effect of combining psyllium fiber with simvastatin in lowering cholesterol. Arch Intern Med. 2005;165(10):1161–6.
Gazi IF, Daskalopoulou SS, Nair DR, Mikhailidis DP. Effect of ezetimibe in patients who cannot tolerate statins or cannot get to the low density lipoprotein cholesterol target despite taking a statin. Curr Med Res Opin. 2007;23(9):2183–92.
Stein EA, Ballantyne CM, Windler E, et al. Efficacy and tolerability of fluvastatin XL 80 mg alone, ezetimibe alone, and the combination of fluvastatin XL 80 mg with ezetimibe in patients with a history of muscle-related side effects with other statins. Am J Cardiol. 2008;101(4):490–6.
Glueck CJ, Aregawi D, Agloria M, et al. Rosuvastatin 5 and 10 mg/d: a pilot study of the effects in hypercholesterolemic adults unable to tolerate other statins and reach LDL cholesterol goals with nonstatin lipid-lowering therapies. Clin Ther. 2006;28(6):933–42.
Backes JM, Moriarty PM, Ruisinger JF, Gibson CA. Effects of once weekly rosuvastatin among patients with a prior statin intolerance. Am J Cardiol. 2007;100(3):554–5.
Gadarla M, Kearns AK, Thompson PD. Efficacy of rosuvastatin (5 mg and 10 mg) twice a week in patients intolerant to daily statins. Am J Cardiol. 2008;101(12):1747–8.
Backes JM, Venero CV, Gibson CA, et al. Effectiveness and tolerability of every-other-day rosuvastatin dosing in patients with prior statin intolerance. Ann Pharmacother. 2008;42(3):341–6.
Juszczyk MA, Seip RL, Thompson PD. Decreasing LDL cholesterol and medication cost with every-other-day statin therapy. Prev Cardiol. 2005;8(4):197–9.
Rivers SM, Kane MP, Busch RS, Bakst G, Hamilton RA. Colesevelam hydrochloride-ezetimibe combination lipid-lowering therapy in patients with diabetes or metabolic syndrome and a history of statin intolerance. Endocr Pract. 2007;13(1):11–6.
Disclosure
Ram Y. Gordon reports no potential conflict of interest relevant to this article. David J. Becker reports no potential conflict of interest relevant to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gordon, R.Y., Becker, D.J. The Role of Red Yeast Rice for the Physician. Curr Atheroscler Rep 13, 73–80 (2011). https://doi.org/10.1007/s11883-010-0145-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11883-010-0145-0