
Abstract
Purpose
Brain metastases (BM) from colorectal cancer (CRC) are rare. As survival increases in patients with metastatic CRC, it is hypothesised that new metastatic patterns will emerge: for instance, as CRC with limited metastatic involvement of the liver and lung can now be successfully resected, we propose that sites, previously rarely involved in metastatic spread, will become more common. The objective of this study was to describe the experience with BM from CRC in a single cancer centre.
Methods
A prospectively compiled database (1988–2012) of patients with CRC treated in a tertiary referral hospital was retrospectively examined. Patients with a histological diagnosis of CRC and radiologically documented BM were included. Clinical information (including patient demographics, primary and metastatic disease factors) was obtained from medical records.
Results
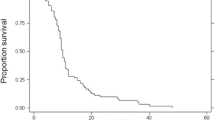
Eleven patients (0.3 % of 4219 patients) were identified (8 male, 3 female). The median age at CRC diagnosis was 70 years (range 55–80 years) while the median age at diagnosis of BM was 73 years (range 56–83 years). Three patients diagnosed with synchronous metastases underwent palliative treatment while eight patients had undergone surgical resection of the primary tumour with curative intent a median of 24 months (range 0–48 months) prior to diagnosis of BM. 10/11 patients were symptomatic at diagnosis of BM. All were diagnosed using computed tomography and managed palliatively. The cerebellum was most the frequently involved site. The median overall survival time following diagnosis of BM was 2.5 months (range 2–9 months). Notably, 8/11 patients were diagnosed in the latter 8 years of the study period (between 2004 and 2012).
Conclusion
With increased survival, improved systemic therapy and aggressive approaches to surgical management of “classical” metastases from CRC, it is likely that a changing pattern of metastases will emerge. As survival rates increase, we propose that metastatic sites, which were previously considered rare (e.g. brain), will now become more common and thus, surgeons must recognise pertinent symptomatology.
Similar content being viewed by others


References
Jemal A et al (2011) Global cancer statistics. CA Cancer J Clin 61(2):69–90
Cancer in Ireland 1994–2011: Annual report of the National Cancer Registry 2014. http://www.ncri.ie/sites/ncri/files/pubs/annual%20report%202014.pdf. Accessed 5 Mar 2014
South and West Cancer Intelligence Unit (2000) Wessex colorectal cancer audit: final report, 5 year outcomes. South and West Cancer Intelligence Unit, Wessex
Wronski M, Arbit E (1999) Resection of brain metastases from colorectal carcinoma in 73 patients. Cancer 85(8):1677–1685
Go PH et al (2011) Gastrointestinal cancer and brain metastasis: a rare and ominous sign. Cancer 117(16):3630–3640
Gavrilovic IT, Posner JB (2005) Brain metastases: epidemiology and pathophysiology. J Neurooncol 75(1):5–14
Sperduto PW et al (2010) Diagnosis-specific prognostic factors, indexes and treatment outcomes for patients with newly diagnosed brain metastases: a multi-institutional analysis of 4259 patients. Int J Radiat Oncol Biol Phys 77:655–661
Tabouret E et al (2012) Recent trends in epidemiology of brain metastases: an overview. Anticancer Res 32(11):4655–4662
Damiens K et al (2012) Clinical features and course of brain metastases in colorectal cancer: an experience from a single institution. Curr Oncol 19(5):254–258
Rees M et al (2008) Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: a multifactorial model of 929 patients. Ann Surg 247(1):125–135
Demmy TL, Dunn KB (2007) Surgical and nonsurgical therapy for lung metastasis: indications and outcomes. Surg Oncol Clin N Am 16(3):579–605 (ix)
Grothey A et al (2004) Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J Clin Oncol 22(7):1209–1214
O’Neill BP et al (2003) A comparison of surgical resection and stereotactic radiosurgery in the treatment of solitary brain metastases. Int J Radiat Oncol Biol Phys 55(5):1169–1176
Jung M et al (2011) Brain metastases from colorectal carcinoma: prognostic factors and outcome. J Neurooncol 101(1):49–55
Onaitis MW et al (2009) Prognostic factors for recurrence after pulmonary resection of colorectal cancer metastases. Ann Thorac Surg 87(6):1684–1688
House MG et al (2010) Survival after hepatic resection for metastatic colorectal cancer: trends in outcomes for 1600 patients during two decades at a single institution. J Am Coll Surg 210(5):744–752 (752–755)
Tomlinson JS et al (2007) Actual 10-year survival after resection of colorectal liver metastases defines cure. J Clin Oncol 25(29):4575–4580
Cardona K et al (2013) Detailed pathologic characteristics of the primary colorectal tumor independently predict outcome after hepatectomy for metastases. Ann Surg Oncol 20(1):148–154
Hess KR et al (2006) Metastatic patterns in adenocarcinoma. Cancer 106(7):1624–1633
Kye BH et al (2012) Brain metastases from colorectal cancer: the role of surgical resection in selected patients. Colorectal Dis 14(7):e378–e385
Sundermeyer ML et al (2005) Changing patterns of bone and brain metastases in patients with colorectal cancer. Clin Colorectal Cancer 5(2):108–113
Farnell GF et al (1996) Brain metastases from colorectal carcinoma. The long term survivors. Cancer 78(4):711–716
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tevlin, R., Larkin, J.O., Hyland, J.M. et al. Brain metastasis from colorectal carcinoma: a single cancer centre experience. Ir J Med Sci 184, 673–675 (2015). https://doi.org/10.1007/s11845-015-1272-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-015-1272-y