
Abstract
Background
The management of patients with chronic pain is challenging. The aim of treatment is alleviation of symptoms in an attempt to increase functional capacity. Interventional procedures, such as chemical neurolysis are adopted when other techniques fail to provide adequate pain control.
Results
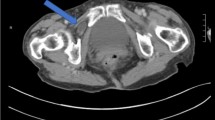
An 82-year-old man presented with a history of chronic left sided abdominal pain. This was initially treated with central nerve blockade. His symptoms persisted and he was scheduled for an intercostal neurolytic block with 6% aqueous phenol. Following the procedure, he experienced further abdominal pain and developed a painful left flank swelling. CT scan, ultrasound scan, and colonoscopy excluded the presence of an organic cause, such as intra-abdominal pathology. A left flank hernia was subsequently diagnosed. Conservative management was employed. Surgical repair will be implemented should conservative measures fail to control symptoms.
Conclusion
This case raises our awareness of a complication that may occur with phenol intercostal neurolysis.


Similar content being viewed by others


References
Healy TEJ, Cohen PJ (1995) Wylie and Churchill-Davidson’s: a practice of anaesthesia, 6th edn. Edward Arnold, London
McQuar HJ, Machin L, Moore RA (1985) Chronic non-malignant pain: a population prevalence study. Practitioner 229:1109–1111
Weksler N, Klein M, Gurevitch B, Rozentsveig V, Rudich Z, Brill S et al (2007) Phenol neurolysis for severe chronic nonmalignant pain: is the old also obsolete? Pain Med 8(4):332–337. doi:10.1111/j.1526-4637.2006.00228.x
American Society of Anesthesiologists Task Force on Pain Management, Chronic Pain Section (1997) Practice guidelines for chronic pain management. A report by the American Society of Anesthesiologists Task Force on Pain Management, Chronic Pain Section. Anesthesiology 86:995–1004. doi:10.1097/00000542-199704000-00032
Burt BM, Afifi HY, Wantz Barie PS (2004) Traumatic lumbar hernia: report of cases and comprehensive review of the literature. J Trauma 57(6):1360–1370. doi:10.1097/01.TA.0000145084.25342.9D
Chatterjee S, Nam R, Fleshner N, Klotz L (2004) Permanent flank bulge is a consequence of flank incision for radical nephrectomy in one half of patients. Urol Oncol 22(1):36–39. doi:10.1016/S1078-1439(03)00099-1
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Al-Hilli, Z., Deasy, J. & Keaveny, J. Flank hernia secondary to phenol nerve block. Ir J Med Sci 179, 451–453 (2010). https://doi.org/10.1007/s11845-009-0312-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-009-0312-x