
Abstract
Purpose
Long arm cast is the method of immobilization after closed reduction of the fracture of the distal third of the forearm, although short arm cast has been used to immobilize the forearm by some orthopedic surgeons. We conducted this study to evaluate the rate of displacement, union time, complication, and cost of treatment between the above-elbow and below-elbow plaster cast groups.
Methods
We designed a prospective randomized controlled trial to compare above- and below-elbow casts for patients of distal forearm fracture aged 4–12 years. One hundred and one patients were presented to our institution during the period from 1st June 2007 to 31st May 2008. Twelve patients were excluded from the study. Eighty-nine patients were randomized into two groups. Four patients were lost to follow up. Hence, 85 patients, 42 in the above-elbow group and 43 in the below-elbow group, were analyzed. Informed consent was obtained prior to participation in the trial. The parameters to be studied were defined before treatment and noted in the pilot-tested pro forma and follow up was done.
Results
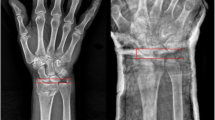
Among the 85 patients analyzed, randomization was successful. Pain and swelling on the next day and at one week following cast application was significantly higher (P = 0.000) in the above-elbow group. Three cases in the above-elbow group needed slitting of the plaster cast. Remanipulation was needed more often in the above-elbow group (9.5%). Although the cast index was not statistically significant (P = 0.054) between the groups, those who needed remanipulation had a larger cast index (0.80). The total cost of the treatment and the number of school days lost was significantly higher (P = 0.000) in the above-elbow group.
Conclusion
Below-elbow cast treatment was comparable in terms of redisplacement, union time, and movement of the wrist to the above-elbow treatment. The complications rate and total cost was higher in the above-elbow plaster group, which could be a cost benefit if a below-elbow cast is used.
Similar content being viewed by others


References
Armstrong PF, Joughlin VE, Clarke HM, Willis RB (1998) Pediatric fracture of the forearm, wrist and hand. In: Greene NE, Swiontkowski MF (eds) Skeletal trauma in children, 3rd edn. Saunders, Philadelphia, pp 166–255
Jones K, Weiner DS (1999) The management of forearm fractures in children: a plea for conservatism. J Pediatr Orthop 19:811–815
Noonan KJ, Price CT (1998) Forearm and distal radius fractures in children. J Am Acad Orthop Surg 6:146–156
Friberg KS (1979) Remodelling after distal forearm fractures in children. I. The effect of residual angulation on the spatial orientation of the epiphyseal plates. Acta Orthop Scand 50:537–546
Friberg KS (1979) Remodelling after distal forearm fractures in children. II. The final orientation of the distal and proximal epiphyseal plates of the radius. Acta Orthop Scand 50:731–739
Friberg KS (1979) Remodelling after distal forearm fractures in children. III. Correction of residual angulation in fractures of the radius. Acta Orthop Scand 50:741–749
Johari AN, Sinha M (1999) Remodeling of forearm fractures in children. J Pediatr Orthop B 8:84–87
Rodríguez-Merchán EC (2005) Pediatric fractures of the forearm. Clin Orthop Relat Res 432:65–72
Chess DG, Hyndman JC, Leahey JL, Brown DC, Sinclair AM (1994) Short arm plaster cast for distal pediatric forearm fractures. J Pediatr Orthop 14:211–213
Bohm ER, Bubbar V, Yong Hing K, Dzus A (2006) Above and below-the-elbow plaster casts for distal forearm fractures in children. A randomized controlled trial. J Bone Joint Surg Am 88:1–8
Webb GR, Galpin RD, Armstrong DG (2006) Comparison of short and long arm plaster casts for displaced fractures in the distal third of the forearm in children. J Bone Joint Surg Am 88:9–17
Price CT, Mencio GA (2001) Injuries to the shafts of the radius and ulna. In: Beaty JH, Kasser JR (eds) Rockwood and Wilkins’ fractures in children, 5th edn. Lippincott Williams & Wilkins, Philadelphia, pp 443–482
Blount WP, Schaefer AA, Johnson JH (1942) Fractures of the forearm in children. JAMA 120:111–116
Davis DR, Green DP (1976) Forearm fractures in children: pitfalls and complications. Clin Orthop Relat Res 120:172–183
Roy DR (1989) Completely displaced distal radius fractures with intact ulnas in children. Orthopedics 12:1089–1092
Borton D, Masterson E, O’Brien T (1994) Distal forearm fractures in children: the role of hand dominance. J Pediatr Orthop 14(4):496–497
Voto SJ, Weiner DS, Leighley B (1990) Redisplacement after closed reduction of forearm fractures in children. J Pediatr Orthop 10:79–84
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Paneru, S.R., Rijal, R., Shrestha, B.P. et al. Randomized controlled trial comparing above- and below-elbow plaster casts for distal forearm fractures in children. J Child Orthop 4, 233–237 (2010). https://doi.org/10.1007/s11832-010-0250-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-010-0250-1