
Abstract
Purpose
Cancer treatment–related late effects degrade survivors’ quality of life, independence, and societal integration, yet may be ameliorated, or even reversed, with effective care. Unfortunately, survivors inconsistently receive this care and the impact on their healthcare utilization is unknown. We sought to estimate differences in utilization between breast cancer (BC) survivors with and without upper extremity lymphedema; a common, remediable late effect.
Methods
We conducted a population-based, retrospective longitudinal cohort study of survivors with incident BC diagnosed from January 1, 1990, through December 31, 2010. HC utilization was characterized using the Berenson-Eggers Type of Service (BETOS) categories. Outcomes included overall healthcare utilization as well as its compartmentalization into the BETOS categories of (1) Evaluation and management, (2) Procedures, (3) Imaging, (4) Tests, (5) Durable medical equipment, (6) Physical/occupational therapy, (7) Other, and (8) Exceptions/Unclassified.
Results
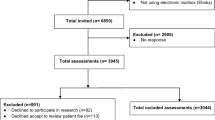
The cohort included 1906 subjects of which 94% (1800) had records meeting the inclusion criteria. Mean follow-up per survivor was 12.8 years (mean, 11, range 1–25 years). Analysis revealed that (1) survivors with BC-associated lymphedema used > 30% more services annually; (2) their increased utilization lessened but persisted for at least 10 years after diagnosis; and (3) this finding of increased utilization extends across all BETOS categories, is further amplified as BMI increases, and cannot be explained solely by lymphedema-directed care.
Conclusions
BC-related lymphedema appears to be an important driver of survivors’ healthcare utilization and guideline-concordant activities to reduce its incidence and severity may be cost neutral or saving.
Implications for Cancer Survivors
Early detection and effective management of cancer-related late effects like lymphedema may reduce survivors’ healthcare needs in the decades that follow their cancer treatment.


Similar content being viewed by others


References
Guy GP Jr, Ekwueme DU, Yabroff KR, et al. Economic burden of cancer survivorship among adults in the United States. J Clin Oncol. 2013;31:3749–57.
Guy GP Jr, Yabroff KR, Ekwueme DU, Rim SH, Li R, Richardson LC. Economic burden of chronic conditions among survivors of cancer in the United States. J Clin Oncol. 2017;35:2053–61.
Ekwueme DU, Yabroff KR, Guy GP Jr, et al. Medical costs and productivity losses of cancer survivors--United States, 2008-2011. MMWR Morb Mortal Wkly Rep. 2014;63:505–10.
Bluethmann SM, Mariotto AB, Rowland JH. Anticipating the “Silver Tsunami”: prevalence trajectories and comorbidity burden among older cancer survivors in the United States. Cancer Epidemiol Biomark Prev. 2016;25:1029–36.
Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66:271–89.
Fernandez-Pineda I, Hudson MM, Pappo AS, Bishop MW, Klosky JL, Brinkman TM, et al. Long-term functional outcomes and quality of life in adult survivors of childhood extremity sarcomas: a report from the St. Jude Lifetime Cohort Study. J Cancer Surviv. 2017;11:1–12.
Hamaker ME, Prins MC, Schiphorst AH, van Tuyl SA, Pronk A, van den Bos F. Long-term changes in physical capacity after colorectal cancer treatment. J Geriatr Oncol. 2015;6:153–64.
Hayes SC, Johansson K, Stout NL, Prosnitz R, Armer JM, Gabram S, et al. Upper-body morbidity after breast cancer: incidence and evidence for evaluation, prevention, and management within a prospective surveillance model of care. Cancer. 2012;118:2237–49.
Soran A, Ozmen T, McGuire KP, et al. The importance of detection of subclinical lymphedema for the prevention of breast cancer-related clinical lymphedema after axillary lymph node dissection; a prospective observational study. Lymphat Res Biol. 2014;12:289–94.
Nesvold IL, Fossa SD, Holm I, Naume B, Dahl AA. Arm/shoulder problems in breast cancer survivors are associated with reduced health and poorer physical quality of life. Acta Oncol. 2010;49:347–53.
Qin ES, Bowen MJ, Chen WF. Diagnostic accuracy of bioimpedance spectroscopy in patients with lymphedema: a retrospective cohort analysis. J Plast Reconstr Aesthet Surg. 2018;71:1041–50.
Johansson K, Branje E. Arm lymphoedema in a cohort of breast cancer survivors 10 years after diagnosis. Acta Oncol. 2010;49:166–73.
Stout NL, Weiss R, Feldman JL, Stewart BR, Armer JM, Cormier JN, et al. A systematic review of care delivery models and economic analyses in lymphedema: health policy impact (2004-2011). Lymphology. 2013;46:27–41.
Shih YC, Xu Y, Cormier JN, Giordano S, Ridner SH, Buchholz TA, et al. Incidence, treatment costs, and complications of lymphedema after breast cancer among women of working age: a 2-year follow-up study. J Clin Oncol. 2009;27:2007–14.
Basta MN, Fox JP, Kanchwala SK, et al. Complicated breast cancer-related lymphedema: evaluating health care resource utilization and associated costs of management. Am J Surg. 2016;211:133–41.
Bar Ad V, Dutta PR, Solin LJ, et al. Time-course of arm lymphedema and potential risk factors for progression of lymphedema after breast conservation treatment for early stage breast cancer. Breast J. 2012;18:219–25.
Specht MC, Miller CL, Russell TA, Horick N, Skolny MN, O’Toole JA, et al. Defining a threshold for intervention in breast cancer-related lymphedema: what level of arm volume increase predicts progression? Breast Cancer Res Treat. 2013;140:485–94.
Rocca WA, Yawn BP, St Sauver JL, Grossardt BR, Melton LJ 3rd. History of the Rochester epidemiology project: half a century of medical records linkage in a US population. Mayo Clin Proc. 2012;87:1202–13.
St Sauver JL, Grossardt BR, Yawn BP, et al. Data resource profile: the Rochester Epidemiology Project (REP) medical records-linkage system. Int J Epidemiol. 2012;41:1614–24.
St Sauver JL, Grossardt BR, Yawn BP, Melton LJ 3rd, Rocca WA. Use of a medical records linkage system to enumerate a dynamic population over time: the Rochester Epidemiology Project. Am J Epidemiol. 2011;173:1059–68.
Melton LJ 3rd, Hartmann LC, Achenbach SJ, Atkinson EJ, Therneau TM, Khosla S. Fracture risk in women with breast cancer: a population-based study. J Bone Miner Res. 2012;27:1196–205.
Cancer AJCo. Breast. AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2010. p. 347–69.
Cheville AL, McGarvey CL, Petrek JA, Russo SA, Thiadens SR, Taylor ME. The grading of lymphedema in oncology clinical trials. Semin Radiat Oncol. 2003;13:214–25.
Fleiss J. Measuring nominal scale agreement among many raters. Psychol Bull. 1971;76:378–82.
Norman SA, Miller LT, Erikson HB, Norman MF, McCorkle R. Development and validation of a telephone questionnaire to characterize lymphedema in women treated for breast cancer. Phys Ther. 2001;81:1192–205.
Sturgeon KM, Dean LT, Heroux M, Kane J, Bauer T, Palmer E, et al. Commercially available lifestyle modification program: randomized controlled trial addressing heart and bone health in BRCA1/2+ breast cancer survivors after risk-reducing salpingo-oophorectomy. J Cancer Surviv. 2017;11:246–55.
Beidas RS, Paciotti B, Barg F, Branas AR, Brown JC, Glanz K, et al. A hybrid effectiveness-implementation trial of an evidence-based exercise intervention for breast cancer survivors. J Natl Cancer Inst Monogr. 2014;2014:338–45.
Norman SA, Localio AR, Potashnik SL, Simoes Torpey HA, Kallan MJ, Weber AL, et al. Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol. 2009;27:390–7.
Sagen A, Karesen R, Sandvik L, Risberg MA. Changes in arm morbidities and health-related quality of life after breast cancer surgery - a five-year follow-up study. Acta Oncol. 2009;48:1111–8.
Armer JM, Radina ME, Porock D, Culbertson SD. Predicting breast cancer-related lymphedema using self-reported symptoms. Nurs Res. 2003;52:370–9.
Togawa K, Ma H, Sullivan-Halley J, et al. Risk factors for self-reported arm lymphedema among female breast cancer survivors: a prospective cohort study. Breast Cancer Res. 2014;16:414.
DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14:500–15.
Dylke ES, Schembri GP, Bailey DL, et al. Diagnosis of upper limb lymphedema: development of an evidence-based approach. Acta Oncol. 2016;55:1477–83.
Bazemore A, Petterson S, Peterson LE, Phillips RL Jr. More comprehensive care among family physicians is associated with lower costs and fewer hospitalizations. Ann Fam Med. 2015;13:206–13.
Mahr MA, Hayes SN, Shanafelt TD, Sloan JA, Erie JC. Gender differences in physician service provision using Medicare claims data. Mayo Clin Proc. 2017;92:870–80.
Zeger SL, Liang KY, Albert PS. Models for longitudinal data: a generalized estimating equation approach. Biometrics. 1988;44:1049–60.
Robins JM. Marginal structural models versus structural nested models as tools for causal inference. In: Halloran ME, Berry D, editors. Statistical models in epidemiology: the environment and clinical trials. New York: Springer; 1999. p. 95–134.
Team RC. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2017.
Secord AA, Hasselblad V, Von Gruenigen VE, et al. Body mass index and mortality in endometrial cancer: a systematic review and meta-analysis. Gynecol Oncol. 2016;140:184–90.
Playdon MC, Bracken MB, Sanft TB, Ligibel JA, Harrigan M, Irwin ML. Weight gain after breast cancer diagnosis and all-cause mortality: systematic review and meta-analysis. J Natl Cancer Inst. 2015;107:djv275.
Hussan H, Gray DM 2nd, Hinton A, Krishna SG, Conwell DL, Stanich PP. Morbid obesity is associated with increased mortality, surgical complications, and incremental health care utilization in the peri-operative period of colorectal cancer surgery. World J Surg. 2016;40:987–94.
Smoot BJ, Wong JF, Dodd MJ. Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: area under the curve. Arch Phys Med Rehabil. 2011;92:603–10.
Rockson SG. Lymphedema after breast cancer treatment. N Engl J Med. 2018;379:1937–44.
Funding
This study was funded by a NCI TREC Survivor Center grant U54-CA155850 from the National Institutes of Health. NCI TREC Survivor Center grant U54-CA155850.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Mayo Clinic Institutional Review Board. The requirement for informed consent was waived for portions of the study that involved retrospective data from clinical records. Informed consent was obtained from surviving cohort members who responded to the survey.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cheville, A., Lee, M., Moynihan, T. et al. The impact of arm lymphedema on healthcare utilization during long-term breast cancer survivorship: a population-based cohort study. J Cancer Surviv 14, 347–355 (2020). https://doi.org/10.1007/s11764-019-00851-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-019-00851-0