
Abstract
Purpose
This study seeks to investigate the long-term public health burden of Hodgkin lymphoma (HL) in terms of work loss following contemporary treatment protocols and associations with established treatment complications and lymphoma relapse.
Methods
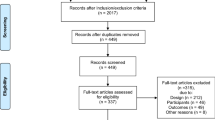
We identified 1,989 Swedish HL patients (1,082 with clinical information) aged 18–60 (median 33) years at diagnosis 1992–2009, and matched 1:4 to population comparators. Sick leave, disability pension (work loss), and comorbidity were retrieved through September 2013. Relative risks (RR) with 95 % confidence intervals (CI) were calculated using Poisson regression, and mean lost work days were estimated yearly during follow-up.
Results
The risk of annual work loss was elevated in HL survivors versus comparators up to the 15th year post-diagnosis (RR5th year 1.64, 95 % CI 1.46–1.84; RR10th year 1.33, 95 % CI 1.15–1.34; and RR15th year 1.30, 95 % CI 1.04–1.62). The risk remained elevated up to the 10th year after adjustment for secondary malignancies and cardiovascular disease (RR10th year 1.31, 95 % CI 1.13–1.52). Advanced-stage patients had more lost days than comparators (mean number5th year 66 versus 33, mean difference 34, 95 % CI 20–48) as did patients receiving 6–8 chemotherapy courses (62 versus 33, mean difference5th year 30, 95 % CI 17–43). Among patients in the first complete remission, a difference was still observed for advanced-stage (51 versus 33, mean difference5th year 19, 95 % CI 5–34) but not early-stage disease.
Conclusions
Advanced-stage HL survivors treated with full-dose chemotherapy were at increased risk of work loss, not only explained by relapse, secondary malignancies, or cardiovascular disease.
Implications for Cancer Survivors
The results call for increased awareness and evaluation of reasons for long-term work disability following intensive chemotherapy among young HL survivors.

Similar content being viewed by others

References
Howlader NNA, Krapcho M, Neyman N, Aminou R, Altekruse SF, Kosary CL, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975–2009 (Vintage 2009 Populations). National Cancer Institute. Bethesda, MD, 2012; Available from: http://seer.cancer.gov/.
Baxi SS, Matasar MJ. State-of-the-art issues in Hodgkin’s lymphoma survivorship. Curr Oncol Rep. 2010;12(6):366–73.
de Boer AG et al. Work ability and return-to-work in cancer patients. Br J Cancer. 2008;98(8):1342–7.
Torp S et al. Change in employment status of 5-year cancer survivors. Eur J Public Health. 2013;23(1):116–22.
Torp S et al. Sick leave patterns among 5-year cancer survivors: a registry-based retrospective cohort study. J Cancer Surviv. 2012;6(3):315–23.
Roelen CA et al. Sickness absence and full return to work after cancer: 2-year follow-up of register data for different cancer sites. Psychooncology. 2011;20(9):1001–6.
Taskila T et al. Comparative study of work ability between cancer survivors and their referents. Eur J Cancer. 2007;43(5):914–20.
Horsboel TA et al. Factors associated with work outcome for survivors from haematological malignancies—a systematic literature review. Eur J Cancer Care (Engl). 2012;21(4):424–35.
Horsboel TA, et al. (2013) Type of hematological malignancy is crucial for the return to work prognosis: a register-based cohort study. J Cancer Surviv 7: 614–623
Horsboel TA, et al. Risk of disability pension for patients diagnosed with haematological malignancies: A register-based cohort study. Acta Oncol. 2014 (in press)
Fobair P et al. Psychosocial problems among survivors of Hodgkin’s disease. J Clin Oncol. 1986;4(5):805–14.
Abrahamsen AF et al. Socio-medical situation for long-term survivors of Hodgkin’s disease: a survey of 459 patients treated at one institution. Eur J Cancer. 1998;34(12):1865–70.
Chen AB et al. Employment and insurance in survivors of Hodgkin lymphoma and their siblings: a questionnaire study. Leuk Lymphoma. 2012;53(8):1474–80.
Mols F et al. Long-term cancer survivors experience work changes after diagnosis: results of a population-based study. Psychooncology. 2009;18(12):1252–60.
Razavi D et al. Professional rehabilitation of lymphoma patients: a study of psychosocial factors associated with return to work. Support Care Cancer. 1993;1(5):276–8.
Bloom JR et al. Psychosocial outcomes of cancer: a comparative analysis of Hodgkin’s disease and testicular cancer. J Clin Oncol. 1993;11(5):979–88.
Barlow L et al. The completeness of the Swedish Cancer Register: a sample survey for year 1998. Acta Oncol. 2009;48(1):27–33.
Amini RM et al. Treatment outcome in patients younger than 60 years with advanced stages (IIB-IV) of Hodgkin’s disease: the Swedish National Health Care Programme experience. Eur J Haematol. 2000;65(6):379–89.
Glimelius I et al. Bulky disease is the most important prognostic factor in Hodgkin lymphoma stage IIB. Eur J Haematol. 2003;71(5):327–33.
Abrahamsson A, Dahle N, Jerkeman M. Marked improvement of overall survival in mantle cell lymphoma: a population based study from the Swedish Lymphoma Registry. Leuk Lymphoma. 2011;52(10):1929–35.
National Board of Health and Welfare. In English–the National Patient Register 2011 Available from: http://www.socialstyrelsen.se/register/halsodataregister/patientregistret/inenglish.
Statistics Sweden. The register of total population. Available from: http://www.scb.se/en_/Finding-statistics/Statistics-by-subject-area/Population/Population-composition/Population-statistics/.
Neovius M, Simard JF, Askling J. How large are the productivity losses in contemporary patients with RA, and how soon in relation to diagnosis do they develop? Ann Rheum Dis. 2011;70(6):1010–5.
National Board of Health and Welfare. Causes of death register. Available from: http://www.socialstyrelsen.se/register/dodsorsaksregistret/bortfallochkvalitet.
Statistics Sweden—LISA database. Background facts, labour and education statistics 2009:1, Integrated database for labour market research. Available from: http://www.scb.se/lisa/.
Thompson SG, Barber JA. How should cost data in pragmatic randomised trials be analysed? BMJ. 2000;320(7243):1197–200.
Hess LM, Insel KC. Chemotherapy-related change in cognitive function: a conceptual model. Oncol Nurs Forum. 2007;34(5):981–94.
Wefel JS, Witgert ME, Meyers CA. Neuropsychological sequelae of non-central nervous system cancer and cancer therapy. Neuropsychol Rev. 2008;18(2):121–31.
Devlen J et al. Psychological problems associated with diagnosis and treatment of lymphomas. II: prospective study. Br Med J (Clin Res Ed). 1987;295(6604):955–7.
Brierley JD et al. Late effects of treatment for early-stage Hodgkin’s disease. Br J Cancer. 1998;77(8):1300–10.
Hellbom M et al. Cancer rehabilitation: a Nordic and European perspective. Acta Oncol. 2011;50(2):179–86.
Beckjord EB et al. Population-level trends in posttreatment cancer survivors’ concerns and associated receipt of care: results from the 2006 and 2010 LIVESTRONG surveys. J Psychosoc Oncol. 2014;32(2):125–51.
Smedby KE. Cancer survivorship and work loss—what are the risks and determinants? Acta Oncol. 2014;53(6):721–3.
Tessaro I et al. Process of diffusing cancer survivorship care into oncology practice. Transl Behav Med. 2013;3(2):142–8.
de Boer AG et al. Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst Rev. 2011;2:CD007569.
de Boer AG, Frings-Dresen MH. Employment and the common cancers: return to work of cancer survivors. Occup Med (Lond). 2009;59(6):378–80.
Kwak L et al. Promoting physical activity and healthy dietary behavior: the role of the occupational health services: a scoping review. J Occup Environ Med. 2014;56(1):35–46.
Neovius K, Neovius M, Rasmussen F. The combined effects of overweight and smoking in late adolescence on subsequent disability pension: a nationwide cohort study. Int J Obes (Lond). 2010;34(1):75–82.
Pryce J, Munir F, Haslam C. Cancer survivorship and work: symptoms, supervisor response, co-worker disclosure and work adjustment. J Occup Rehabil. 2007;17(1):83–92.
Neovius M et al. Patients with ulcerative colitis miss more days of work than the general population, even following colectomy. Gastroenterology. 2013;144(3):536–43.
Ahola K et al. Occupational burnout and medically certified sickness absence: a population-based study of Finnish employees. J Psychosom Res. 2008;64(2):185–93.
de Boer AG et al. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA. 2009;301(7):753–62.
Acknowledgments
This work was supported by the Swedish Cancer Society CAN 2012/774, and the Stockholm County Council 20120169. Karin E Smedby and Martin Neovius were supported by the National Strategic Research Program in Epidemiology in Sweden. Ingrid Glimelius was supported by the Swedish Society of Medicine and the Swedish Society for Medical Research.
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
Conflicts of interest
Ingrid Glimelius, Sara Ekberg, Johan Linderoth, Mats Jerkeman Ellen T Chang, Martin Neovius, and Karin Ekstrom-Smedby declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
sFigure 1
Total number and percentage of lost work days (days of sick leave or disability pension) per year during follow-up among Hodgkin lymphoma patients (register cohort) (A) and population comparators (B). Numbers within bars represent percentages of individuals experiencing work loss during each year, also shown on the y-axis to the left. The mean, 75th and 90th percentile lines refer to the annual number of lost work days shown on the y-axis to the right. Number of patients or comparators contributing with information every other year is listed below the graphs. Sick leave and disability pension data were available from 1994; individuals diagnosed 1992 (patients = 108, comparators = 432) are thus included from the 3rd year (+2y to +3y) and individuals diagnosed in 1993 (patients = 92, comparators = 368) from the 2nd year (+1y to +2y) after diagnosis, which explains why the number of patients and comparators are lower the diagnostic year (dx to +1y) than during the first years of follow-up. (DOCX 1021 kb)
sFigure 2
Mean annual lost work days (days on sick leave or disability pension) among Hodgkin lymphoma patients (register cohort) (A) and population comparators (B). The numbers in/above the bars indicate the mean number of lost work days separately for sick leave and disability pension. The number of individuals contributing with information for complete years of follow-up is indicated below the graph. Sick leave and disability pension data were available from 1994; individuals diagnosed in 1992 (patients = 108, comparators = 432) are thus included from the 3rd year (+2y to +3y) and individuals diagnosed in 1993 (patients = 92, comparators = 368) from the 2nd year (+1y to +2y). (DOCX 199 kb)
sTable 1
(DOCX 13 kb)
sTable 2
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Glimelius, I., Ekberg, S., Linderoth, J. et al. Sick leave and disability pension in Hodgkin lymphoma survivors by stage, treatment, and follow-up time—a population-based comparative study. J Cancer Surviv 9, 599–609 (2015). https://doi.org/10.1007/s11764-015-0436-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-015-0436-0