
Abstract
We report a case of a 51-year-old lady, who underwent a femoral shortening using a fixator assisted blade plate after total hip replacement. The patient had a total hip replacement on the other side with previous revisions, which resulted in a leg length discrepancy. We used the above technique to control the shortening and preserve the mechanical and anatomical axis of the femur.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Case report
A 35-year-old lady with a history of neglected developmental dysplasia (DDH) of the right hip presented with increasing hip pain, back pain and progressive knee deformity. She subsequently underwent conversion of the pseudoarthrosis to a total hip replacement. At the time of surgery, despite adductor tenotomy, it was difficult to relocate the trial prosthesis and a resection of the proximal femur was necessary. A straight stem prosthesis was cemented in the femur (Fig. 1).

AP radiographs of the patient showing neglected congenital dislocation of the right hip and the subsequent primary total hip replacement
Ten years later the patient required a revision of the acetabular component as a consequence of aseptic loosening. The acetabular reconstruction was undertaken using a cemented socket and with impacted bone graft. The reconstruction lasted for 9 more years before a further revision was required. There was extensive bone loss in the acetabulum and the reconstruction was performed using a Burch Schneider support ring, mesh and again with impaction bone graft. The bone stock in the proximal femur was so poor that a proximal femoral allograft with an uncemented stem was used to reconstruct the proximal femur. A leg length discrepancy of 5 cm remained.
Increasingly symptomatic osteoarthritis in the left hip necessitated a left primary arthroplasty to be performed 3 years later. Six months after the left THR (age 51), she presented with increasing back pain attributed to a 5-cm discrepancy in leg length (Fig. 2). Shortening of the left femur was done by performing an external fixator-assisted shortening through a supracondylar resection and internal stabilisation with a blade plate.

AP radiograph of the patient showing limb length discrepancy after having a total hip replacement on the left side
Operative technique
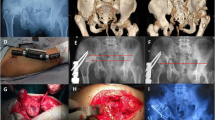
A limb reconstruction system (LRS) external fixator (Orthofix SRL, Italy) with four screws (150/50) was inserted in the sagittal plane under X-ray control perpendicular to the anatomical axis of the femur. Two screws were inserted above and two below the proposed level of femoral resection (Fig. 3). Through a lateral incision and subperiosteal approach a 4-cm segment of the distal femur was removed. The femur was then gradually shortened using the compression–distraction device on the fixator until bone contact at the edges of the osteotomy was achieved. With the fixator still in place, the newly shortened femur was secured using a 9-hole 95°-angled blade plate. The external fixator and its four screws were then removed. The mechanical axis was checked and found to be satisfactory, and the leg length discrepancy reduced to a few millimetres (Fig. 4). The patient made a good postoperative recovery.

Pre-operative planning of the osteotomy and internal fixation using a blade plate

The post-operative radiograph
Discussion
Femoral shortening is a proven method of addressing leg length discrepancy after growth has ceased. The discrepancy should be clinically significant to justify the procedure and should preferably be confined to the femur. The musculature of the femur to be shortened should also be normal. Secure fixation of the osteotomy is essential to allow early joint movement. Options for fixation include internal fixation using plates, intramedullary nailing and external fixation. It is important to maintain femoral alignment and rotation in the shortening.
Treatment of complete developmental dysplasia (congenital dislocation, DDH) of the hip with total hip replacement (THR) in adults is a challenging surgical procedure due to the distorted anatomy and leg length inequality. Correction of the leg length discrepancy may be performed concurrently at the time of arthroplasty or addressed post-operatively. The successful placement of the acetabular component demands an anatomic reduction so as to avoid excessive compressive loads across the hip joint. In order to accomplish this flexor and abductor muscles may be released from the iliac bone as suggested by Harley and Wilkinson [1].
The incidence of nerve palsy in the literature following total hip arthroplasty in DDH is 5–17% [2–7]. In order to avoid excessive nerve stretching, shortening of the proximal femoral metaphysis has been recommended [6–8] and sometimes combined with a trochanteric transfer. However, this shortening and the subsequent leg length discrepancy may jeopardize the longevity of the prosthesis [6, 7, 9, 10] and can adversely affect an otherwise excellent outcome of the THR [7, 11–13].
Most patients with limb-length discrepancy following total hip arthroplasty have manageable symptoms. Further surgery may be indicated after failure of conservative treatment for continuing recurrent instability and significant functional impairment (abductor weakness, dysfunctional gait, or low back pain) [14]. Anwar and Sugan [15] reported a leg length discrepancy greater than 2 cm in 22 patients (total number 34) after THR following DDH.
There is a paucity of published data regarding the outcome of surgical intervention for femoral shortening following THR for DDH. This presents a particular problem since the presence of a THR affects both lengthening and shortening strategies. Parvizi et al. [14] reported 21 cases of revision arthroplasty for the treatment of leg length discrepancy following THR. There was significant improvement in the Harris Hip score, with only one complication of symptomatic subluxation. Sener et al. [16] described 23 cases using a step-cut shortening osteotomy on the long side with stabilization by cerclage cables. After surgery 19 had a leg length discrepancy of less than 2 cm and the remainder exceeded this threshold.
The use of an external fixator and lengthening through the distal femur may entail an unacceptable infection risk and shortening on the long side is to be preferred. However, with the presence of a THR on the long side the options for shortening are limited. Resection and diaphyseal shortening using a supracondylar nail or diaphyseo-metaphyseal shortening using plate fixation remain the options. Care should be taken to avoid a stress riser in the area between the two implants. In this case report the use of a fixator-guided technique conferred certain advantages: (1) controlled gradual shortening; (2) control of rotation; (3) control over the axis of the femur; and (4) stable temporary fixation whilst the blade plate was inserted. To our knowledge this method of femoral shortening after total hip replacement has not been previously reported.
Through pre-operative planning and intra-operative templating, any tendency to medialise the mechanical axis of the limb as a result of shortening along the anatomical axis of the femur may be identified and corrected prior to plate insertion. In general terms such a correction is probably only necessary for larger amounts of shortening and/or when a significant varus deformity is present pre-operatively.
References
Harley JM, Wilkinson JA (1987) Hip replacement for adults with unreduced congenital dislocation. A new surgical technique. J Bone Joint Surg Br 69:752–755
Crowe JF, Mani VJ, Ranawat CS (1979) Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am 61:15–23
Davlin LB, Amstutz HC, Tooke SM, Dorey FJ, Nasser S (1990) Treatment of osteoarthrosis secondary to congenital dislocation of the hip. Primary cemented surface replacement compared with conventional total hip replacement. J Bone Joint Surg Am 72:1035–1042
Jensen JS, Retpen JB, Arnoldi CC (1989) Arthroplasty for congenital hip dislocation. Techniques for acetabular reconstruction. Acta Orthop Scand 60:86–92
Johanson NA, Pellicci PM, Tsairis P, Salvati EA (1983) Nerve injury in total hip arthroplasty. Clin Orthop 179:214–222
Song KM, Halliday SE, Little DG (1997) The effect of limb-length discrepancy on gait. J Bone Joint Surg Am 79:1690–1698
Williamson JA, Reckling FW (1978) Limb length discrepancy and related problems following total hip joint replacement. Clin Orthop 134:135–138
Dunn HK, Hess WE (1976) Total hip reconstruction in chronically dislocated hips. J Bone Joint Surg Am 58:838–845
Gofton JP (1971) Studies in osteoarthritis of the hip. IV. Biomechanics and clinical considerations. Can Med Assoc J 104:1007–1011
Ilstrup DM, Nolan DR, Beckenbaugh RD, Coventry MB (1973) Factors influencing the results in 2,012 total hip arthroplasties. Clin Orthop 95:250–262
Bose WJ (2000) Accurate limb-length equalization during total hip arthroplasty. Orthopedics 23:433–436
Edeen J, Sharkey PF, Alexander AH (1995) Clinical significance of leg-length inequality after total hip arthroplasty. Am J Orthop 24:347–351
Ranawat CS, Rodriguez JA (1997) Functional leg-length inequality following total hip arthroplasty. J Arthroplasty 12:359–364
Parvizi J, Sharkey PF, Bissett GA, Rothman RH, Hozack WJ (2003) Surgical treatment of limb-length discrepancy following total hip arthroplasty. J Bone Joint Surg Am 85-A:2310–2317
Anwar MM, Sugano N, Masuhara K, Kadowaki T, Takaoka K, Ono K (1993) Total hip arthroplasty in the neglected congenital dislocation of the hip. A five- to 14-year follow-up study. Clin Orthop 295:127–134
Sener N, Tozun IR, Asik M (2002) Femoral shortening and cementless arthroplasty in high congenital dislocation of the hip. J Arthroplasty 17:41–48
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kasis, A.G., Stockley, I. & Saleh, M. External fixator-assisted acute shortening with internal fixation for leg length discrepancy after total hip replacement. Strat Traum Limb Recon 3, 35–38 (2008). https://doi.org/10.1007/s11751-008-0031-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11751-008-0031-2