
Abstract
Healthcare-associated pneumonia (HCAP) has been proposed as a new category of pneumonia distinct from community-acquired pneumonia (CAP). A multicenter observational study in 2008 finds that patients with HCAP have a mortality rate significantly higher than patients with CAP, and a worse outcome is associated at logistic regression analysis with a low adherence to empirical antibiotic therapy recommended by ATS/IDSA guidelines. We designed a prospective interventional study to establish whether administration of a broad-spectrum antibiotic therapy consistent with the 2005 ATS/IDSA guidelines has an effect on the clinical outcome of hospitalized patients with HCAP. All patients with HCAP prospectively admitted in 25 medical wards of 20 Italian hospitals during a 1-month period were included in the study. All patients were assigned to receive an empirical therapy including a fluoroquinolone plus an anti-MRSA agent plus either piperacillin–tazobactam or a carbapenem. Main measures for improvement were duration of antibiotic therapy, length of hospital stay, and in-hospital mortality rate. Patients were compared with a historical control group of 90 patients, and followed up to discharge or death. HCAP patients receiving a guideline-concordant therapy had a shorter duration of antibiotic therapy (median 15 vs. 12 days, p = 0.0002), a shorter duration of hospitalization (median 18 vs. 14 days, p = 0.02), and a lower mortality rate (17.8 vs. 7.1 %, p = 0.03). Our results suggest that an empirical broad-spectrum therapy is associated with improved outcome in patients with HCAP.
Similar content being viewed by others

Introduction
Classically, pneumonia represents a spectrum of diseases that range from community-acquired to hospital-acquired and ventilator-associated pneumonia. The 2005 American Thoracic Society (ATS)/Infectious Diseases Society of America (IDSA) guidelines [1] incorporated for the first time the new concept of healthcare-associated pneumonia (HCAP) that includes patients who have recent or chronic contact with health care system, such those living in nursing homes, attending hemodialysis clinics, receiving parental therapy in the 30 days before pneumonia, or with a history of recent hospitalization within 90 days). Several studies have provided original data about this topic [2–12], and the published literature suggests that patients with disease that falls under the HCAP definition have a significantly higher in-hospital mortality than those classified as having “true” CAP. The increased mortality seems to be associated with a greater likelihood to receive an inappropriate empirical antibiotic therapy [2, 8, 11–14], and one critical disparity between the two groups of patients appears to be a higher incidence of infection with multi-drug resistant (MDR) pathogens in the HCAP group [1, 11, 12, 15–18].
For the initial empirical treatment of patients with HCAP, the 2005 ATS/IDSA guidelines recommend the administration of broad-spectrum antibiotics [1]. This is the same strategy as that recommended for patients with hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP), both groups with risk factors for MDR pathogens. In a multicenter, prospective observational study [13], we ascertained the epidemiology and outcome of CAP, HCAP and HAP in adult patients hospitalized in Italian internal medicine wards. Compared with patients who had CAP, patients with HCAP have a greater severity of clinical conditions, a significantly higher mean duration of antibiotic therapy, a higher length of hospital stay, and higher mortality rates. At multivariate analysis, the receipt of an empirical antibiotic therapy not recommended by international guidelines is the main factor independently associated with increased intra-hospital mortality [OR 6.4 (CI 2.3–17.6)].
The present study is a multicenter interventional study evaluating the clinical effectiveness of an empirical broad-spectrum antibiotic therapy for the treatment of HCAP.
Patients and methods
Setting and period of study
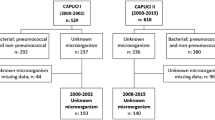
We planned a multicenter study in those divisions of internal medicine to evaluate the clinical effectiveness of an empirical broad-spectrum antibiotic therapy for the treatment of HCAP. To this end, we performed a before–after study by comparing a prospective interventional group with an historical one. The interventional study was performed in 25 divisions of internal medicine in 20 Italian hospitals during a 1-month period (1–28 February 2009). Prior to the start of the study, at least one physician from each center participated in a single-day investigator meeting. Participating centers were geographically distributed across various regions of the North, Central or South of Italy. All patients enrolled in the study were compared with a group of 90 patients with HCAP enrolled in a previous prospective observational study (historical control group). Cases of pneumonia of the latter group were assessed during two active 1-week surveillance study periods (22–29 January and 25 June–2 July 2007). All the physicians who participated in the interventional study took part in the first study that enrolled the patients of the historical control group.
The study was done in accordance with the International Conference on Harmonization guidelines on Good Clinical Practice and the principles of the Declaration of Helsinki. The study was registered on the website of the Italian Medicines Agency (Osservatorio Nazionale per la Sperimentazione dei Medicinali, AIFA), EudraCT number 2009-016476-67, and was approved by the independent ethics committee or institutional review board at all participating institutions. The study comprised only adult patients (>18 years) with HCAP who were hospitalized in internal medicine wards during a 4-week period (1 February–1 March 2010).
Patients
Our inclusion criteria were radiologic evidence of pneumonia, and at least two of the following criteria: fever or hypothermia (temperature >38 °C or <35 °C), dyspnea, cough and purulent sputum, pleuritic chest pain, or signs of consolidation on respiratory auscultation. We classified patients as having HCAP if they had been admitted to an acute-care hospital for at least 2 days in the prior 180 days, or resided in a long-term care facility (LTCF), or had attended a hospital or hemodialysis clinic, or had received intravenous therapy (included antibiotics) in the prior 30 days [13]. Exclusion criteria included acquisition of pneumonia in the intensive care unit (ICU) or in another hospital and HIV infection.
Measurements
To stratify patients into risk classes, we used the prediction rule calculated according to the PSI and the CURB-65 scores. We recorded the following data: age, gender, intrinsic and extrinsic risk factors, clinical signs and symptoms, results from laboratory studies, chest radiography pattern, results of microbiologic studies, antibiotic therapy, and outcome. Severity of clinical conditions was assessed at the time of presentation using the SOFA score.
Microbiological studies
All patients included in the study underwent the following diagnostic procedures: blood cultures, Legionella pneumophila serogroup 1 antigen in urine, and sputum culture (if available). Further studies such as S. pneumoniae antigen in urine, standard serologic methods to determine antibodies against atypical agents, pleural fluid culture, or culture of bronchoalveolar lavage (BAL) were performed on the basis of the availability of the above-mentioned methods or according to the judgment of the attending physician.
Microbiological data were culture results from the first 48 h after admission to hospital. An etiologic diagnosis was considered definitive if one of the following criteria was met: (1) blood cultures yielded a bacterial pathogen (in the absence of an apparent extrapulmonary focus); (2) pleural fluid and transthoracic needle aspiration culture yielded a bacterial pathogen; (3) respiratory sample representative of the lower respiratory tract (fiberoptic bronchoscopy with protected catheter) yielded a bacterial pathogen; (4) isolation of L. pneumophila in sputum or detection of L. pneumophila serogroup 1 or pneumococcal antigen in urine; (5) fourfold increase in the antibody titer, or seroconversion for atypical pathogens. An etiologic diagnosis was considered presumptive when a predominant microorganism was isolated from a purulent sputum sample [presence of >25 polymorphonuclear leukocytes and <10 squamous cells per low-power field (original magnification ×10)] with compatible Gram’s stain findings. Presumptive aspiration pneumonia was diagnosed on a clinical and radiological basis in patients who had risk factors such as compromised consciousness, altered gag reflex, dysphagia, severe periodontal disease, putrid sputum, or necrotizing pneumonia in absence of positive respiratory specimens cultures.
The following pathogens were considered as multi-drug resistant (MDR): methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum β-lactamase (ESBL) producing Gram-negative Enterobacteriaceae, Pseudomonas aeruginosa, Acinetobacter baumannii, Stenotrophomonas maltophilia and other Enterobacteriaceae spp. resistant for three or more of the following antibiotic classes: antipseudomonal cephalosporins or penicillins, carbapenems, fluoroquinolones and aminoglycosides.
Antimicrobial treatment
All patients with diagnosis of HCAP were assigned to receive an empirical antibiotic therapy as follows: a fluoroquinolone (ciprofloxacin 400 mg i.v. every 8 h or levofloxacin 750 mg i.v. every 24 h) plus an anti-methicillin-resistant Staphylococcus aureus (MRSA) agent (vancomycin 1 g i.v. every 12 h or linezolid 600 mg i.v. every 12 h) and either an antipseudomonal β-lactam (piperacillin–tazobactam 4.5 g i.v. every 8 h) or a carbapenem (imipenem 500 mg i.v. every 6 h or meropenem 1 g i.v. every 8 h). Drug dosages were modified according to the creatinine clearance calculated using the Cockroft–Gault formula. Dose adjustments of vancomycin based on renal function and vancomycin serum concentrations were left to the individual judgment of the clinicians at the different study sites. Treatment was performed for at least 7 days; a prolonged treatment was given if deemed necessary by the attending physician. Treatment was discontinued if any underlying disease or infection was exacerbated, efficacy of treatment was inadequate, or the condition was exacerbated, incidental symptoms developed, adverse reactions or laboratory abnormalities developed, the patient or his/her proxy requested discontinuation, or if the attending physician considered discontinuation necessary for other reasons. In cases in which an etiological diagnosis was obtained, antibiotic therapy was de-escalated on the basis of microbiological results.
Statistical analysis
Data are presented as median values (interquartile range) for quantitative variables and as absolute and relative frequencies (95 % CI) for categorical variables. Data obtained in the study group (interventional group) were compared with a historical control represented by 90 patients prospectively investigated in a previous study [13, 19]. We performed the Mann–Whitney U test for comparisons between quantitative variables and the Pearson Chi-square test or the generalized Fisher exact test for contingency table analysis. We investigated the association between in-hospital mortality (as outcome variable) and all the other collected variables using multivariate logistic regression. We used the Hosmer–Lemeshow methodology for variable selection as previously reported [19]. All the significant variables were put into the final model of multivariate logistic regression analysis. We performed the Pearson goodness-of-fit test to assess the overall fit of the model. We computed odds ratios (ORs) derived from the covariates, and their confidence intervals using a clustered robust standard error estimation. A cluster includes all the cases from one participating ward. Relationships between the primary outcome variable and each of the continuous ones were investigated by fractional polynomial logistic regression analysis; continuous variables were eventually transformed accordingly before being put into the multivariate regression model. A 2-tailed p value of less than 0.050 was considered statistically significant for all the analyses. We used STATA/SE, version 9.2 for Windows (StataCorp, College Station, TX, USA), to analyze the data.
Results
In total, 127 subjects with HCAP who were admitted to the study hospitals were included in the study. The median age was 78 years (range 18–100 years) and 54.3 % of the patients were men. The backgrounds of the 127 patients are shown in Table 1.
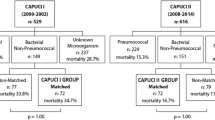
Table 2 shows clinical characteristics of 90 patients included in the historical control group and 127 in the intervention group. Overall, patients did not significantly differ in terms of median age, sex distribution, underlying diseases, clinical or laboratory findings. The only differences were represented by a higher incidence of heart failure (p = 0.009) and bilateral involvement at chest radiograph (p = 0.01) in the historical control group, while renal failure was more frequent in the intervention group (p = 0.04). Three patients (3.3 %) of the first group and five patients (4.2 %) of the second group received non-invasive mechanical ventilation.
Table 3 summarizes microbiological findings. There were no differences in the percentage of patients with established etiological diagnosis (31.1 vs. 32.3 %) between study groups. S. aureus was the most common pathogen (39.3 vs. 24.4 %), and the rate of methicillin resistance was 63.6 % in the pre-intervention and 70 % in the intervention group. Gram-negative bacilli were also frequent, mainly represented by Enterobacteriaceae (31.7 % of cases) and, less frequently, by P. aeruginosa (12.2 %). Among Enterobacteriaceae species isolated, 69.2 % were ESBL-producing strains (5 Klebsiella spp., 2 E. coli, 2 E. cloacae), and additionally one Morganella spp., one Enterobacter cloacae and one Klebsiella ozenae were classified as MDR.
Table 4 describes the risk stratification of patients calculated by use of PSI and CURB-65 scores. Most patients of both groups were included in the high-risk classes of PSI (IV and V) and CURB-65 (class III) severity scores. However, patients of the intervention group had significantly higher mean values of their PSI score (p < 0.01). Table 5 describes the antibiotic regimens administered in patients with HCAP of the historical control group. Table 6 shows data on antimicrobial therapy and outcomes of the two HCAP groups. Among patients included in the intervention group, vancomycin (83.5 %) was the more common anti-MRSA agent used, piperacillin/tazobactam (81.1 %) was the most prevalent anti-Gram-negative agent (meropenem 10.2 %, imipenem 8.7 %), while levofloxacin (77.2 %) was the most commonly fluoroquinolone used. Vancomycin treatment was discontinued in five cases (3.9 %) for renal toxicity and substituted with linezolid, levofloxacin was discontinued in two cases and ciprofloxacin in one case for allergic reactions. Compared to patients included in the historical control group, those included in the intervention group had a shorter duration of antibiotic therapy (median 15 vs. 12 days, p = 0.0002, a shorter duration of hospitalization (median 18 vs. 14 days, p = 0.02), and a lower mortality rate (17.8 vs. 7.1 %, p = 0.03).
Figure 1 shows ORs and 95 % confidence intervals of the variables that were significantly and independently associated with in-hospital mortality at the multivariate logistic regression analysis.

Factors independently associated with in-hospital mortality at multivariate logistic regression analysis (only significant variables are shown in this final model)
Discussion
The first goal of our study was a “real-time” analysis of the clinical approaches of physicians attending hospitalized patients with HCAP with the aim of evaluating the efficacy of a new treatment protocol. The 2005 ATS/IDSA guidelines [1] incorporated for the first time the new concept of HCAP that includes patients who have recent or chronic contact with health care system, such as those living in nursing homes, attending hemodialysis clinics, receiving parental therapy in the 30 days before pneumonia, or with a history of recent hospitalization within 90 days. The findings of our study suggest that administration of a broad-spectrum empirical therapy, including MRSA and potentially MDR Gram-negative bacilli coverage, is associated with shorter hospital stay (mean 18 vs. 14 days; p = 0.03), shorter duration of antibiotic therapy (mean 15 vs. 12 days; p < 0.0002), and lower mortality rates (17.8 vs. 7.1 %; p = 0.03). These results seem to confirm a benefit of the antibiotic strategy recommended for HAP/VAP among patients with HCAP.
A recent review discussed the evidence supporting the role of MDR bacteria in patients with HCAP, and the strength of the evidence for the individual risk factors linking them with the presence of MDR pathogens [15]. Different international studies [2, 6–9, 11] seem to share the message that a percentage of patients with HCAP have a high likelihood of receiving an inappropriate empirical antibiotic therapy due to a greater risk of infection with MDR pathogens. However, the major limitation of these studies is that an etiologic diagnosis was performed only in a minority of patients with HCAP (about 30–40 % of cases in the published articles), and also our prospective study identified the causative pathogens only in about 30 % of cases. Thus, microbiological data from patients with culture-positive pneumonia could not be representative of all cases of HCAP.
The concept of HCAP may be much more complex and heterogeneous than to date believed, and many authors have expressed concern that antibiotic treatment decisions driven by the concept of HCAP might lead to excessive prescription and abuse of broad-spectrum anti-infectives [20] leading to unnecessary costs and promote resistance. To address this limitation of the HCAP concept, Shorr and collegues hypothesize that a risk-score approach is more accurate than the complete HCAP definition, and, consequently, would result in fewer patients being given broad-spectrum antibiotic therapy unnecessarily [21]. They assign points as follows: 4 for recent hospitalization, 3 if presenting from a LTC facility, 2 if chronic HD, 1 if admitted to the ICU within 24 h of evaluation in the ED, for a possible maximum score of 10. Analyzing retrospectively a cohort including 977 patients, the authors find that as the score increases, the probability of recovering a resistant organism also increases. As a screening test for resistant organisms, a score = 0 has a high negative predictive value (84.5 %) and leads to fewer patients unnecessarily receiving broad-spectrum antibiotics. Similarly, Aliberti and colleagues [22] evaluated, in a prospective study, risk factors for acquiring MDR bacteria among patients coming from the community who were hospitalized with pneumonia. The authors, moreover, evaluated patients’ clinical outcome during hospitalization, and developed a risk- scoring tool to identify subjects with pneumonia caused by MDR organisms. A total of 935 patients with pneumonia were enrolled in the study of whom 437 (51 %) had at least 1 risk factor for acquiring MDR bacteria on admission. Among all risk factors, hospitalization in the preceding 90 days (OR 4.87) and residency in a nursing home (OR 3.55) are independent predictors for an actual infection with a resistant pathogen. A simple score ranging from 0 to 12.5 and performed on admission to the hospital was used to stratify patients into different classes based on the probability of having MDR pneumonia. Among patients with a score ≤0.5 on entry (low risk class), the prevalence of a resistant bacteria is 8 % (95 % CI 2–13 %), compared with 38 % (95 % CI 25–50 %) in those with a score of ≥3 (p < 0.001). These recent studies may, in part, explain the successful outcome observed in our interventional study group, since more than 90 % of our patients, on the basis of risk factors, had high values of Shorr and Aliberti risk scores, and thus high probability of MDR pathogens. This finding is probably related to the fact that we analyzed only patients admitted to Internal Medicine wards, who are usually older and more disabled than those hospitalized in other medical wards.
In addition, a low incidence of etiological diagnosis in HCAP patients may be, in part, explained by a significant percentage of infections by anaerobic bacteria, which are not routinely cultured in respiratory specimens. All previously published studies report that HCAP patients are usually older, more disabled, and with multiple risk factors for aspiration pneumonia, such as deterioration of consciousness, or need for a feeding tube. A previous study analyzing swallowing function reports a high incidence of aspiration pneumonia among hospitalized patients with a history of prior hospitalization for at least 2 days in the preceding 90 days or a stay at a nursing home or LTCF [23]. A high incidence (20.6 %) of probable aspiration pneumonia is also documented in the studies of Carratalà [2] and Shindo (58.2 %) [11]. HCAP patients appear then at high risk for infections by anaerobic bacteria, and a misdiagnosed high incidence of aspiration pneumonia due to anaerobic bacteria may explain the improved outcome observed in our study since all patients received a β-lactam with extended activity against anaerobic pathogens (piperacillin–tazobactam or a carbapenem). Most antibiotics recommended for the treatment of CAP (such as third-generation cephalosporin, macrolides, or levofloxacin) do not ensure adequate anti-anaerobic coverage. The patients included in the historical control group had a higher incidence of heart failure, and the presence of bilateral involvement on chest radiograph; both these conditions may affect survival in CAP patients [24], and thus may be, in part, responsible for the increased mortality observed in the historical control group. However, at regression logistic analysis, these factors were not significantly associated with poor outcome.
The design of this study and the use of an historical control group as comparator may also, in part, explain the improved clinical outcome observed in the intervention group of patients. The before–after study is the most common design encountered in quality improvement research, but many potentially relevant changes may occur between “before” and “after” periods of measurement. For example, all physicians included in the prospective interventional study initially received scientific materials discussing the epidemiology and outcome of HCAP, then participated in an educational event leading to a better understanding of the correct clinical approach to patients with CAP and HCAP. Participants were also skilled about diagnostic procedures, drug dosages, and adjustment of drugs in the presence of a reduced creatinine clearance. The primary goal of our study was an evaluation of the clinical approaches of physicians attending hospitalized patients with HCAP, with an aim of recognizing incorrect behaviors, and to evaluate the efficacy of the new ATS/ISDA recommendations. In this regard, our study confirms the benefit of educational programs for quality improvement in clinical practice. However, the pneumonia severity index at admission was greater in the intervention group than in the historical control group, and such difference would probably strengthen the results of our study, reducing the risk of misleading results.
To compare the interventional group with the historical one, we used 180 days as a cut-off for recent hospitalization to differentiate between CAP and HCAP. This is different from ATS criteria (hospitalization in the preceding 90 days), and may be another potential limitation of our study. The choice of expanding the inclusion criteria for HCAP was based on a number of considerations, including the prolonged duration of colonization and possible subsequent infections with resistant bacteria (e.g., S. aureus) after hospital discharge [24–26]. The importance of a prolonged bacterial colonization was also suggested by a retrospective cohort study involving 639 patients with culture-positive CAP and HCAP admitted to a single center, which revealed how patients who were hospitalized for 2 or more days in the preceding 12 months were also at risk for MDR pathogens.
In conclusion, our investigation provides important insights into developing local strategies for treating patients with HCAP. We found that among patients at high risk for MDR pathogens, a broad-spectrum empirical approach may be associated with improved outcome and reduction in the length of hospitalization. A significant percentage of patients with HCAP enrolled in a multicenter national study (about 50 %) had an infection by MDR pathogens, or an aspiration pneumonia. This epidemiological situation seems to warrant an empirical coverage of these pathogens until culture results are available. Our results suggest the importance of recognition of risk factors for MDR pathogens in patients with HCAP to administer an appropriate empirical antibiotic treatment.
References
American Thoracic Society and the Infectious Diseases Society of America (2005) Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 171:388–416
Carratalà J, Mykietiuk A, Fernández-Sabé N, Suárez C, Dorca J, Verdaguer R, Manresa F, Gudiol F (2007) Healthcare-associated pneumonia requiring hospital admission: epidemiology, antibiotic therapy, and clinical outcomes. Arch Intern Med 167:1393–1399
Cecere LM, Rubenfeld GD, Park DR, Root RK, Goss CH (2010) Long-term survival after hospitalization for community-acquired and healthcare-associated pneumonia. Respiration 79:128–136
Falcone M, Serra P, Licata G, Venditti M, The Italian Society of Internal Medicine (SIMI) (2008) Healthcare-associated pneumonia: a new clinical entity. Arch Intern Med 168:109–110
Hsu JL, Siroka AM, Smith MW, Holodniy M, Meduri GU (2011) One-year outcomes of community-acquired and healthcare-associated pneumonia in the Veterans Affairs Healthcare System. Int J Infect Dis. 15:e382–e387
Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS (2005) Epidemiology and outcomes of healthcare-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest 28:3854–3862
Labelle AJ, Arnold H, Reichley RM, Micek ST, Kollef MH (2010) A comparison of culture-positive and culture-negative healthcare-associated pneumonia. Chest 137:1130–1137
Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH (2007) Healthcare-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother 51:3568–3573
Rello J, Luján M, Gallego M, Vallés J, Belmonte Y, Fontanals D, Diaz E, PROCORNEU Study Group (2010) Why mortality is increased in Healthcare-associated Pneumonia: lessons from pneumococcal bacteremic pneumonia. Chest 137:1138–1144
Schreiber MP, Chan CM, Shorr AF (2010) Resistant pathogens in non-nosocomial pneumonia and respiratory failure: is it time to refine the definition of healthcare-associated pneumonia? Chest 137:1283–1288
Shindo Y, Sato S, Maruyama E, Ohashi T, Ogawa M, Hashimoto N, Imaizumi K, Sato T, Hasegawa Y (2009) Healthcare-associated pneumonia among hospitalized patients in a Japanese community hospital. Chest 135:633–640
Shorr AF, Zilberberg MD, Micek ST, Kollef MH (2008) Prediction of infection due to antibiotic-resistant bacteria by select risk factors for healthcare-associated pneumonia. Arch Intern Med 168:2205–2210
Venditti M, Falcone M, Corrao S, Licata G, Study Group of the Italian Society of Internal Medicine (2009) Outcomes of patients hospitalized with community-acquired, healthcare-associated, and hospital-acquired pneumonia. Ann Intern Med 150:19–26
Zilberberg MD, Shorr AF, Micek ST, Mody SH, Kollef MH (2008) Antimicrobial therapy escalation and hospital mortality among patients with healthcare-associated pneumonia: a single-center experience. Chest 134:963–968
Falcone M, Venditti M, Shindo Y, Kollef MH (2011) Healthcare-associated pneumonia: diagnostic criteria and distinction from community-acquired pneumonia. Int J Infect Dis. 15:e545–e550
Falcone M, Venditti M, Corrao S, Serra P, The Italian Society of Internal Medicine (SIMI) Study Group (2011) Role of multidrug-resistant pathogens in healthcare-associated pneumonia. Lancet Infect Dis. 11:11–12
Jung JY, Park MS, Kim YS, Park BH, Kim SK, Chang J, Kang YA (2011) Healthcare-associated pneumonia among hospitalized patients in a Korean tertiary hospital. BMC Infect Dis 11:61
Shindo Y, Hasegawa Y (2011) Emerging problems regarding severity assessment and treatment strategies for patients with pneumonia: controversies surrounding the HCAP concept. Intern Emerg Med 6:389–391
Falcone M, Corrao S, Venditti M, Serra P, Licata G (2011) Performance of PSI, CURB-65, and SCAP scores in predicting the outcome of patients with community-acquired and healthcare-associated pneumonia. Intern Emerg Med 6:431–436
Brito V, Niederman MS (2009) Healthcare-associated pneumonia is a heterogeneous disease, and all patients do not need the same broad-spectrum antibiotic therapy as complex nosocomial pneumonia. Curr Opin Infect Dis. 22:316–325
Shorr AF, Zilberberg MD, Reichley R et al (2012) Validation of a clinical score for assessing the risk of resistant pathogens in patients with pneumonia presenting to the emergency department. Clin Infect Dis 54:193–198
Aliberti S, Di Pasquale M, Zanaboni AM et al (2012) Stratifying risk factors for multidrug-resistant pathogens in hospitalized patients coming from the community with pneumonia. Clin Infect Dis 54:470–478
Teramoto S, Fukuchi Y, Sasaki H, Sato K, Sekizawa K, Matsuse T (2008) High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: a multicenter, prospective study in Japan. J Am Geriatr Soc 56:577–579
Minne L, Ludikhuize J, de Rooij SE, Abu-Hanna A (2011) Characterizing predictive models of mortality for older adults and their validation for use in clinical practice. J Am Geriatr Soc 59:1110–1115
Scanvic A, Denic L, Gaillon S, Giry P, Andremont A, Lucet JC (2001) Duration of colonization by methicillin-resistant Staphylococcus aureus after hospital discharge and risk factors for prolonged carriage. Clin Infect Dis 32:1393–1398
Falcone M, Serra P, Venditti M (2009) Serious infections due to methicillin-resistant Staphylococcus aureus: an evolving challenge for physicians. Eur J Intern Med 20:343–347
Acknowledgments
This study was part of an independent research program of the Italian Society of Internal Medicine, and was not funded by any organization.
Conflict of interest
None.
Ethical approval
Obtained.
Author information
Authors and Affiliations
Corresponding author
Additional information
On behalf of the Italian Society of Internal Medicine (SIMI).
The participating members of The Italian Society of Internal Medicine (SIMI) are given in Appendix.
Appendix
Appendix
Participating members of The Italian Society of Internal Medicine (SIMI): Giovanni Battista Bianchi, Silvia Curri (Ospedale SS Gerosa e Capitanio, Lovere), Francesco Violi, Stefania Basili, Alessandro Russo, Antonio Vena (Policlinico Umberto I-Università di Roma “La Sapienza”), Maria Rosaria Pirro, Filippo Alegiani (Ospedale Fatebenefratelli Isola. Tiberina, Roma), Antonio Cerqua, Daniele Pignata, Francesca Fanfarillo, Paolo Carfagna (Azienda Ospedaliera San Giovanni Addolorata, Roma); Luigi Calvo (Policlinico Universitario “A Giaccone”, Palermo); Mauro Bernardi, Silvia Li Bassi, Alessandro Principe (Policlinico S. Orsola Malpighi, Bologna), Salvatore Antonaci, Francesco Saverio Vella, Stefania Pugliese, Carmela Giannatempo (Policlinico Università di Bari); Roberto Manfredini, Susanna Gamberini (Ospedale del Delta, Lagosanto Ferrara), Ranuccio Nuti, Roberto Valenti (Azienda Ospedaliera Universita degli Studi di Siena); Gianfranco Guarnieri, Michela Zanetti (Ospedale di Cattinara, Trieste); Nicola Lucio Liberato (Ospedale Civile, Casorate Primo); Pier Mannuccio Mannucci, Elisa Giglio, Walter Monzani, Anna Maria Brambilla (Policlinico Ospedale Maggiore, Milano); Carlo Balduini, Gino Roberto Corazza (Fondazione IRCCS Policlinico San Matteo-Università di Pavia); Massimo Vanoli, Gianluca Casella (Ospedale di Lecco-P.O. di Merate); Alfonso Noto, Elio Fiaschi (Ospedale Civile dell’Annunziata, Cosenza); Giuseppe Musca (Ospedale G. Iannelli Cetraro) Giovanni Gasbarrini, Pietro Tilli, Nicolò Gentiloni Silveri (Università Cattolica del Sacro Cuore, Policlinico A. Gemelli, Roma); Alessandro Lechi, Germana Montesi (Policlinico G.B. Rossi, Verona), Giuseppe Realdi, Nicola Vitturi (Azienda Ospedaliera, Padova). Nicoletta Luchena (Ospedale di Putignano)
Rights and permissions
About this article
Cite this article
Falcone, M., Corrao, S., Licata, G. et al. Clinical impact of broad-spectrum empirical antibiotic therapy in patients with healthcare-associated pneumonia: a multicenter interventional study. Intern Emerg Med 7, 523–531 (2012). https://doi.org/10.1007/s11739-012-0795-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-012-0795-8