
Abstract
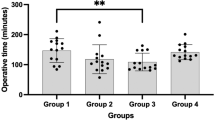
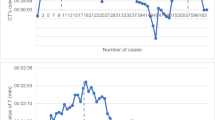
It has been suggested that up to 40 cases of RALP are required to reach the operative results equal to open surgery. We have hypothesized that previous experience in open and laparoscopic surgeries might shorten the learning curve of robotic surgery. We have retrospectively evaluated the data of all children who underwent pyeloplasty in our institute by a single surgeon since 2003. The children were divided into three groups: open pyeloplasty (OP) of 72 children, laparoscopic pyeloplasty (LAP) of 22, and RALP of 33 patients subsequently. The data included: demographics, duration of surgery, length of stay, success of surgery, and complication rate according to the Clavien–Dindo score. The groups were ordered chronologically by the operation date and each group was divided into two different phases: early and late. A comparison was made between the data of the early and the late phase. There was no difference in the demographic data between the groups; however, the patients who underwent laparoscopic surgery were significantly older compared with the patients from the other groups. The median duration of surgery in the RALP group was significantly shorter than the OP group (65 min vs 72.5 min P < 0.01), while the first RALP case was already shorter than the median duration of surgery in OP group. There was no significant decrease in the duration of surgery of the RALP group over the study period, though there was a significant trend of decreasing operative time in the OP and LAP groups. There was no difference in the length of stay in the early vs late phases in the RALP group. There was no difference in the complication and success rate between the RALP and OP group, as well as the early and late phases of the RALP group. Our data show that previous experience in OP and LAP surgery may contribute to a shorter learning curve of robotic surgery required for the surgeon to achieve a similar outcome to that of OP.



Similar content being viewed by others

Availability of data and material
Not applicable.
Code availability
Not applicable.
References
Chertin B, Pollack A, Koulikov D, Rabinowitz R, Hain D, Hadas-Halpren I, Farkas A (2006) Conservative treatment of ureteropelvic junction obstruction in children with antenatal diagnosis of hydronephrosis: lessons learned after 16 years of follow-up. Eur Urol 49(4):734–739
Kafka IZ, Kocherov S, Jaber J, Chertin B (2019) Pediatric robotic-assisted laparoscopic pyeloplasty (RALP): does weight matter? Pediatr Surg Int 35(3):391–396
Nguyen HT, Herndon CD, Cooper C, Gatti J, Kirsch A, Kokorowski P et al (2010) The Society for Fetal Urology consensus statement on the evaluation and management of antenatal hydronephrosis. J PediatrUrol 6(3):212e31
Vemulakonda VM, Hamer MK, Kempe A, Morris MA (2019) Surgical decision-making in infants with suspected UPJ obstruction: stakeholder perspectives. J Pediatr Urol 15(5):469
Lee RS, Retik AB, Borer JG, Peters CA (2006) Pediatric robot assisted laparoscopic dismembered pyeloplasty: comparison with a cohort of open surgery. J Urol 175(2):683–687
Tasian GE, Wiebe DJ, Casale P (2013) Learning curve of robotic assisted pyeloplasty for pediatric urology fellows. J Urol 190(4):1622–1627
Sorensen MD, Delostrinos C, Johnson MH, Grady RW, Lendvay TS (2011) Comparison of the learning curve and outcomes of robotic assisted pediatric pyeloplasty. J Urol 185(6S):2517–2522
Cundy TP, Gattas NE, White AD, Najmaldin AS (2015) Learning curve evaluation using cumulative summation analysis—a clinical example of pediatric robot-assisted laparoscopic pyeloplasty. J Pediatr Surg 50(8):1368–1373
Kassite I, Braik K, Villemagne T, Lardy H, Binet A (2018) The learning curve of robot-assisted laparoscopic pyeloplasty in children: a multi-outcome approach. J Pediatr Urol 14(6):570–e1
Scarlett AL, Mentessidou A, Farrugia MK, De Caluwé D, Rahman N (2019) Urology robotic journey: demonstrating the learning curve in robot-assisted pyeloplasties (RALP). J Pediatr Endosc Surg 1(2):79–82
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
David Dothan, Galia Raisin, Jawdat Jaber, Stanislav Kocherov, and Boris Chertin declare that they have no conflict of interest.
Ethics approval
We received approval from the institute review board.
Informed consent
Consent to participate: not applicable. Consent for publication: not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dothan, D., Raisin, G., Jaber, J. et al. Learning curve of robotic-assisted laparoscopic pyeloplasty (RALP) in children: how to reach a level of excellence?. J Robotic Surg 15, 93–97 (2021). https://doi.org/10.1007/s11701-020-01082-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-020-01082-7