
Abstract
Introduction
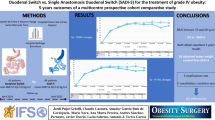
Single-anastomosis duodenal switch has been suggested to be an effective bariatric procedure that offers excellent weight loss and by lengthening the common channel the potential to reduce micronutrient deficiencies.
Purpose
To evaluate the weight loss, comorbidity resolution and the 1-year nutritional outcomes of the single-anastomosis duodenal switch (SADS) procedure.
Setting
Multiple US Hospitals.
Methods
From October 2014 to January 2017, 120 patients were enrolled at six sites across the USA and underwent the SADS procedure. Weight loss, comorbidities, quality of life, and adverse events were followed post-procedure for 12 months.
Results
At 1, 6, and 12 months, 98.3%, 85.5%, and 77.1% of the patients were available for assessment, respectively. At 12 months, patients showed significantly reduced body mass index when compared to baseline (46.8 ± 5.8 vs 29.8 ± 4.4, P < 0.001 respectively). Sixty-five patients had type 2 diabetes at baseline; however, 11 patients lost to follow-up. Of the available data (54 patients), 96.3% of the patients had a resolution of type 2 diabetes by 12 months with a mean A1C reduction from 7.8 ± 1.6 to 5.3 ± 0.7. Additionally, there were reductions in hyperlipidemia, sleep apnea, and hypertension at 12 months. Patient gastroesophageal reflux disease satisfaction and quality of life (SF-36) scores were significantly higher at 12 months post-procedure (P < 0.001 in all cases) while 12-month protein levels remained at normal values. There were abnormalities of parathyroid hormone and vitamin D at 1 year with all other nutritional markers being not significantly different at 1 year from baseline. There were 10, IIIb, or greater complications according to the Clavien-Dindo scoring system during the study period, not all of which were related to the surgery.
Conclusions
SADS is a highly efficacious weight loss procedure with significant comorbidity reduction at 1 year. At 1 year, complications and vitamin and mineral deficits appear to be consistent with other malabsorption operations. Long-term follow-up is needed, especially around complications and vitamin deficiencies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although bariatric surgery is the most effective treatment for class II and III obesity, the optimal procedure remains elusive. Procedures such as biliopancreatic diversion (BPD) and duodenal switch (DS) offer the greatest weight loss but have been plagued by concerns of protein and vitamin deficiency. The Roux-en-Y gastric bypass (RYGB) has been the most common procedure that combines a gastric and intestinal approach. Although effective, concerns include marginal ulcer, small-bowel obstruction, and reactive hypoglycemia. Additionally, for those with super morbid obesity, weight loss is often less than optimal [1,2,3]. The vertical sleeve gastrectomy (VSG) has become the most common stapling procedure. Although it is suggested that VSG has fewer complications, there are increasing reports of inadequate weight loss and weight regain. As a result, if there was a procedure that could offer superior weight loss and minimize the risk of malnutrition, it would be a valuable addition to the bariatric community.
The laparoscopic duodenal switch (LDS) has better long-term weight loss and diabetes resolution when compared to RYGB and VSG [4]. However, concerns about its protein calorie malnutrition have slowed its adoption. Several authors have reported on a variation where a calibrated vertical sleeve gastrectomy is combined with a single anastomosis to the bowel 3 m from the ileocecal valve [5,6,7]. This prospective multi-center study was designed to evaluate the weight loss, comorbidity resolution, and the 1-year nutritional outcomes of the single-anastomosis duodenal switch (SADS) procedure.
Methods
Trial Design
The trial protocol was approved at each institution’s institutional review board in accordance with the Helsinki declaration. All patients signed informed consent to participate. The study protocol is available with the full text of this article at NEJM.org. The study was included in the Clinicaltrials.gov Protocol Registration System (NCT02275208).
According to the protocol, the study required 120 patients in total. From October 2014 through January 2017, 120 patients who agreed to take part in the study were enrolled at six sites across the USA. Inclusion criteria were an age of 18–65, BMI of 35–40 kg/m2 with one obesity-related comorbidity, or a BMI of 40–60 kg/m2. Exclusion criteria included any female patient who was pregnant or breast feeding, any patient part of a vulnerable population, or any previous bariatric surgery. Patients who had an estimated life expectancy of less than 6 months, or who had participated in an investigational drug or device research study within 30 days of enrollment, were also not included.
Each site had a dedicated research team for data collection. The QOL data were gathered by researchers. But the serious adverse events (SAEs) were both reported by the surgeon and verified by the research teams. The research teams also audited each chart for unknown SAEs at the end of the study.
Trial Outcomes
The primary endpoint was weight loss as seen in percent excess weight loss (%EWL; calculated from an ideal body weight (IBW) using NIH guidelines), percent total body weight loss (%TWL; calculated from preoperative body weight), and patients final BMI at 1 year.
The secondary end points were (1) incidence of procedure-related adverse events through 12 months postoperatively; (2) quality of life (SF-36) assessed preoperatively, and 6 and 12 months; (3) gastroesophageal reflux disease health-related quality of life (GERD-HRQL) (10) questionnaire preoperatively and at 6 and 12 months; (4) incidence of pre-procedure vitamin deficiencies; (5) incidence of post-procedural vitamin deficiencies at 1, 6, and 12 months; and (6) resolution of comorbidities evaluated at 1, 6, and 12 months. Resolutions for comorbidities are defined as follows: type 2 diabetes (T2D)—achieving A1C level ≤ 6% and a fasting blood glucose < 126 mg/dl with or without the use of medications; hypertension—achieving blood pressure < 140/90 mmHg or the presence of blood pressure lowering medications; sleep apnea was diagnosed by a sleep study by a sleep specialist prior to having surgery. This workup was not part of the protocol. This was discovered as part of the history of the patient. If the individual site felt the patient needed a workup, they would be referred to a sleep specialist. However, this was solely at the discretion of the study site. Sleep apnea was considered cured if treatment was discontinued by a sleep specialist (i.e., no need for continuous positive airway pressure); hyperlipidemia—total cholesterol of < 200 mg/dl, LDL cholesterol < 130 mg/dl; and hypertriglyceridemia—triglyceride < 150 mg/dl.
Trial Oversight
Medtronic supported this investigator initiated trial. Statistical analysis of the data was performed under the direction of the lead investigators of the study (Roslin, Cottam) with statisticians employed by Medtronic. Each site had access to their own data and verified its accuracy and their adherence to trial protocol.
Treatments
The operations were performed per standard of care and as previously described by Mitzman et al. [5]. In brief, retrograde tracing and tacking of the small bowel (300 cm), sleeve creation, duodenal dissection and transection, and duodeno-ileostomy (DI) were performed. Sleeve gastrectomy was performed over a sizing tube (40–46 French), and the distance from the pylorus was around 3 to 5 cm. The proximal duodenum was transected approximately 3 cm distal to the pylorus. A loop DI was performed at approximately 300 cm from the ileocecal valve. At each center, a totally hand-sewn technique was used, but the choice of single- or double-layer technique and type of suture was left to each individual surgeon [8] (Fig. 1). The Petersen’s defect was not closed in any of the cases.

Single-anastomosis duodenal switch (SADS) procedure anatomical schematic
Patients were maintained on a liquid diet for the first postoperative month. In addition, multivitamin supplements, calcium, and iron were prescribed. All the patients are recommended to take ADEK multivitamins, calcium citrate 1800/2400 mg/day, iron 65 mg/day, and daily protein intake 60–80 g/day. Prior to the procedure and at 6- and 12-month follow-ups, patients completed both a SF-36 and a GERD-HRQL questionnaire [9, 10]. The total score of all questions as well as subject satisfaction levels were compared pre- and postoperatively.
Comorbidity and Laboratory Analyses
Preoperatively and 1, 6, and 12 months postoperative comorbidities and relevant lab tests (e.g., glucose, hemoglobin, A1C, hematocrit, ferritin, albumin, total protein, calcium, parathormone, vitamin A, vitamin B1, vitamin B12, vitamin D, folic acid, insulin and lipid panel, triglycerides, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), C-peptides, iron, copper, and zinc) per standard of care were assessed.
Statistical Analysis
For excess weight loss %, total weight loss %, and BMI loss %, a two-sided one sample t test was used to test whether the mean change from baseline was significant for each postoperative visit. For SF-36, a two-sided Wilcoxon signed rank test was used to test whether the mean change from baseline was significant. Univariate ANCOVA was done for each unique variable accrued to test for independent variable affecting weight loss. Analyses were performed using SAS® Version 9.4 or higher (SAS Inc., Cary, NC).
Results
Trial Patients
One hundred thirty (130) patients were consented for the study. Nine patients were screen failures (provided consent however was deemed ineligible before procedure) and one patient withdrew before the surgery. One hundred twenty procedures were started; however, two could not be completed. At 1, 6, and 12 months, 116 (98.3%), 101 (85.5%), and 91 (77.1%) patients were available for assessment respectively. Reasons for follow-up loss included pregnancy, relocation, and subject withdrawal. This follow-up loss happened despite each center having one person assigned to follow-up each individual at each time point.
The groups’ demographic information included 67.8% females with an average age of 46.2 ± 10, a mean weight of 134.1 ± 2 0.4 kg, and a BMI of 47.4 ± 5.7 kg/m2 (Table 1).
Primary Outcome; Weight Loss
Patients showed consistent weight loss through time as seen in %EWL, %TWL, and reduction of BMI (Table 1). With univariate analysis, operation site and individual comorbid conditions did not play a role in weight loss. Only the bundle of diabetes, hypertension, and sleep apnea together showed a decrease in weight loss outcomes (Table 2).
Secondary Outcomes
Comorbidities
Type 2 Diabetes
T2D was present in 65 of 118 patients preoperatively (55%, defined as an A1C > 6.5 without medications or any patient currently taking medications for T2D as prescribed by their primary care physician). The mean A1C was 7.8 ± 1.6 preoperative (Table 3). Of the 65 patients, 27 (42%) were insulin-dependent diabetics. Eleven diabetic patients were lost to follow-up. Of the remaining 54 patients, T2D was resolved (A1C ≤ 6 without medications) or controlled (A1C ≤ 6 with medications) in 96% of diabetics with a mean A1C level of 5.3. Only two patients of the 27 on insulin had A1C levels of greater than 6.0 at 1 year (7.1 and 7.0). Ninety-three percent of insulin-dependent diabetics had a A1C < 6 at 125 1 year with or without medications.
Lipid Profiles
Preoperatively 40% of patients were on medications for hyperlipidemia (Table 3) and 49% of patients had elevated LDL. Postoperatively through 12 months, only 3.7% of patients had elevated total cholesterol and only 20% of patients had elevated LDL. Eight patients on hyperlipidemia medications and 18 with elevated LDL were lost to follow-up. Medication declined by half through the 1-year study from 40% preoperatively to 16% at 12 months. HDL increased throughout the study from a mean of 42.8 preoperatively to 48.6 at 1 year (Table 3).
Sleep Apnea
Sleep apnea affected 59.3% of the patients at baseline and at 1 year only 30.8% reported having sleep apnea (Table 3). For the study, resolution of sleep apnea was defined as all sleep apnea treatment discontinued (i.e., no need for continuous positive airway pressure.
Hypertension
Hypertension was present in 61.9% of patients preoperatively (Table 3). Of the 73 patients who had preoperative hypertension, 66% had resolved by 1 year (no antihypertensive medications) and had a normal blood pressure measured during office assessment.
GERD-HRQL results
Eighty of 118 patients who started the study had GERD evaluations (GERD-HRQL questionnaire) completed at all time points. Although this group represents approximately 70% of the total population, it is believed to be representative and would not introduce bias. Of this group, 21(26%) had severe and ongoing daily GERD symptoms preoperatively. At 1 year, only seven of 80 patients had ongoing GERD. Of these seven, two had GERD that did not change, four had new onset GERD that was significant, and one improved but was still positive for GERD symptoms. Overall, 81% of patients with GERD symptoms preoperatively had complete GERD resolution without hiatal hernia repair.
Fifty-nine of the 80 patients who started the study did not have any GERD symptoms. Of these, only 5% developed new onset GERD. None of the patients who experienced worsening GERD had a hiatal hernia repair done at the time of surgery.
Overall patient GERD satisfaction rose significantly by 12 months postoperatively when compared to baseline, peaking with 95% of the 80 patients saying they were satisfied or neutral at 12 months. This differs markedly from preoperative data where only 34% said they were satisfied with their GERD symptoms.
Quality of Life
Assessed preoperatively and at 6 and 12 months postoperatively, patients demonstrated significant increases in all aspects of SF-36 quality of life survey with physical functioning showing the greatest increase (50.7 ± 25.01 vs. 86.9 ± 21.02) and mental health showing the lowest increase (69.4 ± 19.25 vs. 80.7 ± 17.92) at 12 months (Table 3).
Nutritional Data
Assessments of the minerals copper, zinc, and ferritin showed that at 1 year, there were mineral deficiencies of 3.4%, 0%, and 16.5% respectively. Calcium, another mineral, is always studied with parathormone. Preoperatively, there were deficiencies in calcium in two patients and one patient parathormone level. At 1 year, there was one patient with a calcium deficiency and 43% of patients had an elevated parathormone level.
Of the fat-soluble vitamins, preoperatively, vitamin D had the most deficiencies with only 47% of patients having normal values and 53% having insufficiency or deficiency. At 1 year, little had changed with 55% having insufficiency or deficiency with 44.8% being normal. Vitamins E and A had 1% and 0% preoperative deficiencies, respectively, while at 1 year the data looked similar with 0% and 1% deficiencies respectively. Vitamin K was deficient in 18% of patients preoperatively and at 1 year the data was similar with 24% of patients deficient.
There were two longer term malnutrition markers evaluated: total protein and albumin. 3.6% of patients had low total protein preoperatively with 4.6% at 1 year while albumin was abnormal in 1% of patients preoperatively and 5% at one year.
Safety and Adverse Events
Of 118 patients who completed the SADS procedure, 30 experienced procedure-related events. Events were reviewed and graded on the Clavien-Dindo scale [11]. In total, there were 20 minor complications and nine major complications (Tables 4 and 5). A single patient was grade 5, death as the result of cardiac arrest 90 months postoperatively which was not procedure related. Additionally, we counted laparoscopic cholecystectomies as complications of the procedure. In addition, 4 months postoperatively one patient had a chylous fistula which has not been reported in the literature previously as a complication of bariatric surgery. Of note was the only unique complication of the procedure which was an abnormal filling of an afferent limb that was related to the loop configuration.
Discussion
The primary objective of bariatric surgery was weight loss. In this study in which patients had a starting mean BMI of 47 kg/m2, 53% of subjects achieved a BMI < 30 at 1 year. As this was a clinical registry without comparison group, it is complex to place this outcome in perspective. Previously, the Michigan collaborative reported a rate of only 36% of patients achieving a BMI < 30 kg/m2 in a large cohort that underwent bariatric surgery within the state. It is important to highlight that 16% of the patients had laparoscopic adjustable gastric banding (LAGB) and this may have had a negative effect. The mean BMI of patients that reached a BMI < 30 kg/m2 was 42 kg/m2. [12]. In our study, 10 of 21 patients (48%) with a BMI of > 50 kg/m2 were able to reduce their body weight to < 30 compared to 8% from the Michigan collaborative. For patients with BMI > 50 kg/m2, less than 5% had LAGB in the collaborative. While not directly comparable, there are certain insights that can be obtained, it appears that SADS might offer greater weight loss and may be an attractive option for patients with higher BMIs whose objective is to no longer be obese. Importantly, patients who reach levels that are no longer obese have a reduced incidence of recidivism and derive more lasting control of their comorbid conditions. In our study, operation site was not a factor in weight loss outcomes (P = 0.131, Table 2).
An important point to decipher is diabetes resolution. The population studied had a preoperative A1C of 7.8. Forty-two percent of the patients studied were on insulin. With SADS, 52 of 54 diabetic patients had an A1C < 6.0 mg/dl at 1 year (96%). Of these patients, four were still on medication and thus cannot be counted as having complete remission. For perspective, in the stampede trial, only 38% of RYGB patients and 24% of VSG patients reached a similar threshold [13]. As these were not matched populations, no conclusion can be drawn. However, our study shows that SADS is an effective procedure for type 2 diabetes. In a study by Cottam et al., a direct comparison was made between SADS and RYGB [14]. The study had a 3-year follow-up data, and they found SADS to be more effective in treating the T2DM than RYGB. In a recent study by Enochs et al., the A1C values between these two procedures were compared [15]. It was found that the SADS had significantly lower rates of abnormal A1C than RYGB at 12 months. Again, we cannot make a definite conclusion as there is no long-term data available in the literature comparing these two procedures. Future trials that directly compare the procedures with matched populations, as well as with long-term outcomes, are required before any statement of comparative effectiveness can be made.
Operations that bypass the intestine will provide the greatest weight loss, but this is always with the risk of micronutrient deficiency. Despite these patients’ large size, the presence of deficiencies in morbid obese individuals prior to surgery is common. In our study, nearly 50% of our subjects were vitamin D deficient prior to surgery. While it is preferable to treat these deficiencies preoperatively and replete patients prior to surgery, this was not done. Patient labs were drawn very close to the surgical procedure and deficient vitamin D was not felt to be a reason to delay the bariatric procedure. This was the standard practice at all the sites. In retrospect, it would have been best to get assessments earlier and begin repletion prior to surgery. Numerous patients in our study actually had an increase in vitamin D postoperatively. Thus, many could absorb their supplements. It is not known whether patients with deficiency were not compliant with their vitamin or the procedure interfered with absorption. It is promising that the deficiency rate was identical to the preoperative level. Close attention to fat-soluble vitamin levels is mandatory following this procedure. If this procedure grows in popularity, there may be a role for regular parenteral fat-soluble vitamins or transdermal application.
There has long been a concern about calcium absorption in operations that bypass parts of the small intestine. In this study, there was only a single patient with calcium deficiency at 1 year. This is in stark contrast to other studies when looking at calcium in gastric bypass, where serum calcium has been low. It has long been believed that low calcium levels are the main driver of elevated PTH serum values after malabsorptive surgery [16]. However, our study, while the short term, suggests that this is not the case, and other mechanisms are driving the elevated PTH seen in our patients.
When looking at PTH levels, 43% elevated at 1 year seems high, especially since it has been reported more than once that PTH levels can rise with long-term follow-up [16,17,18,19,20,21]. A further concern is that these elevated PTH levels will lead to bone fracture and osteopenia. When we compare our outcome to others in the literature, we find that the standard RYDS has a range of elevated PTH levels between 45 and 60%. Gastric bypass has a range between 5 and 88.9% [16,17,18,19]. A single paper of one anastomosis gastric bypass (OAGB) has shown a 72% of patients had elevated PTH following surgery [22]. In comparison to these other procedures, our levels at 1 year seem consistent with other malabsorption procedures. Since our levels were similar to gastric bypass, a comparison of gastric bypass to SADS is warranted. Axelsson et al. indicated in his seminal paper on the subject of fractures after gastric bypass that for gastric bypass, “fracture risk appeared to increase with time [23]. The risk of fall injury without fracture was also increased after gastric bypass. Larger weight loss or poor calcium and vitamin D supplementation after surgery were not associated with increased fracture risk.” Clearly, we would expect that our results would parallel these findings of 38,000 Swedish patients. Yet, Axxelson et al. demonstrated very convincingly that the simple relationship between calcium, vitamin D, and PTH for fractures does not exist, and more need to be done to decide what markers, if any, can predict fracture and what supplementation can stop it [23].
Despite the fact that this operation bypassed the duodenum, we had no incidence of iron deficiency anemia. Likewise, our rate of other micronutrient deficiencies remained low at 1 year. The sum of these results indicates that preserving 3 m of intestine provides an adequate conduit for the majority of patients to successfully absorb cations and fat-soluble vitamins. These results suggest that patients who eat proper foods and take suggested supplements can maintain acceptable levels of protein, vitamins, and minerals. Another concern is quality of life. During the course of the study, there was an improvement in every aspect of the SF-36. Patient satisfaction rose from 31% preoperatively to 80% at one year.
Any intervention has complications. In our series, there were 30 adverse events. The performance of a SADS is a complex bariatric procedure. It is technically more challenging than VSG and less surgeons are familiar than RYGB. Additionally, the mean BMI of this cohort was 48 with a high propensity of type 2 diabetes. Exact comparison is impossible but it is our belief that rates were comparable or less than historical reports with other bariatric procedures. Complications associated with the sleeve creation were similar to primary vertical sleeve gastrectomy (VSG). It is our hope that these can be vastly reduced with better education and experience. As a result, there is potential to lower the risk of stricture and leak. In a study by Surve et al., the reported duodeno-ileostomy (DI) leak rate in 1328 SADS patients was 0.6% [7]. Interestingly, none of our patients experienced leak at the DI.
Only one complication was related to the loop configuration where there was preferential flow into the afferent limb [24]. This was treated by laparoscopy and a pexy stitch to prevent backflow. The single death in the study was unrelated to surgery and was from heart failure in a patient with pre-existing heart disease (Tables 4 and 5).
There has been a transition in procedure preference. VSG has increased with lap band disappearing and RYGB declining. An issue with VSG is GERD [25,26,27]. Using a standard GERD-HQRL questionnaire, 81% of patient with GERD preoperatively had resolution of their symptoms and only 4% developed de novo symptoms. This was remarkable and surprised the authors of the paper. Unfortunately, this data was not available for all 118 patients (only 80 completed the GERD-HQRL at all time points) and we cannot say what happened in those patients who did not fill out the survey at all time points. It is hoped that comparative trials in the future will focus on GERD difference between VSG and SADS with emphasis on preoperative EGD and biopsy results.
There are limitations in this study. Perhaps the most glaring is concerning our T2DM resolution. There is no denying that our results were excellent and much better than RYGBP. However, true comparisons are hard, especially as we did not gather data on length of diabetes pre op. Additionally, we suffered from a lack of a comparative cohort and only 1-year follow-up. Additionally, there were patients lost to follow-up. Sadly, this was not due to lack of resources as each site had an individual dedicated to following these individuals and we still lost 23% of patients at 1 year which makes it adequate for reporting but not ideal.
Because of these issues, only general conclusions can be drawn.
Conclusion
In this multi-center trial, we were able to show that SADS is an effective weight loss operation and that it can reduce comorbid conditions without causing protein malabsorption at 1 year. Long-term follow-up papers are needed to address many issues surrounding this procedure.
References
Eisenberg D, Azagury DE, Ghiassi S, et al. ASMBS Position Statement on postprandial hyperinsulinemic hypoglycemia after bariatric surgery. Surg Obes Relat Dis. 2017;13(3):371–8.
Kim J, Brethauer S, Committee ACI, et al. Metabolic bone changes after bariatric surgery. Surg Obes Relat Dis. 2015;11(2):406–11.
Obeid NR, Malick W, Concors SJ, et al. Long-term outcomes after Roux-en-Y gastric bypass: 10- to 13-year data. Surg Obes Relat Dis. 2016;12(1):11–20.
Hess DS, Hess DW, Oakley RS. The biliopancreatic diversion with the duodenal switch: results beyond 10 years. Obes Surg. 2005;15(3):408–16.
Mitzman B, Cottam D, Goriparthi R, et al. Stomach Intestinal pylorus sparing (sips) surgery for morbid obesity: retrospective analyses of our preliminary experience. Obes Surg. 2016;26(9):2098–104. https://doi.org/10.1007/s11695-016-2077-4.
Surve A, Zaveri H, Cottam D, et al. A retrospective comparison of biliopancreatic diversion with duodenal switch with single anastomosis duodenal switch (SIPS-stomach intestinal pylorus sparing surgery) at a single institution with two year follow-up. Surg Obes Relat Dis. 2017;13(3):415–22.
Surve A, Cottam D, Sanchez-Pernaute A, et al. The incidence of complications associated with loop duodeno-ileostomy after single-anastomosis duodenal switch procedures among 1328 patients: a multicenter experience. Surg Obes Relat Dis. 2018 May;14(5):594–601.
Surve A, Zaveri H, Cottam D. A safer and simpler technique of duodenal dissection and transection of the duodenal bulb for duodenal switch. Surg Obes Relat Dis. 2016;12(4):923–4. https://doi.org/10.1016/j.soard.2016.02.022.
Velanovich V. The development of the GERD-HRQL symptom severity instrument. Dis Esophagus. 2007;20(2):130–4.
Ware Jr JE. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130–9.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Varban OA, Cassidy RB, Bonham A, et al. Factors associated with achieving a body mass index of less than 30 after bariatric surgery. JAMA Surg. 2017;152(11):1058–64. https://doi.org/10.1001/jamasurg.2017.2348.
Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes-3-year outcomes. N Engl J Med. 2014;370(21):2002–13. https://doi.org/10.1056/NEJMoa1401329.
Cottam A, Cottam D, Zaveri H, et al. An analysis of mid-term complications, weight loss, and type 2 diabetes resolution of stomach intestinal pylorus-sparing surgery (SIPS) versus Roux-en-Y gastric bypass (RYGB) with three-year follow-up. Obes Surg. 2018 Sep;28(9):2894–902.
Enochs P, Bull J, Surve A, et al. Comparative analysis of the single-anastomosis duodenal-ileal bypass with sleeve gastrectomy (SADI-S) to established bariatric procedures: an assessment of 2-year postoperative data illustrating weight loss, type 2 diabetes, and nutritional status in a single US center. Surg Obes Relat Dis. In press
Johnson JM, Maher JW, DeMaria EJ, et al. The long-term effects of gastric bypass on vitamin D metabolism. Ann Surg. 2006;243(5):701–4. discussion 704-5
Jin J, Robinson AV, Hallowell PT, et al. Increases in parathyroid hormone (PTH) after gastric bypass surgery appear to be of a secondary nature. Surgery. 2007;142(6):914–20. discussion 914-20
Hewitt S, Søvik TT, Aasheim ET, et al. Secondary hyperparathyroidism, vitamin D sufficiency, and serum calcium 5 years after gastric bypass and duodenal switch. Obes Surg. 2013 Mar;23(3):384–90.
Johnson JM, Maher JW, Samuel I, et al. Effects of gastric bypass procedures on bone mineral density, calcium, parathyroid hormone, and vitamin D. J Gastrointest Surg. 2005;9(8):1106–10. discussion 1110-1
Switzer NJ, Marcil G, Prasad S, et al. Long-term hypovitaminosis D and secondary hyperparathyroidism outcomes of the Roux-en-Y gastric bypass: a systematic review. Obes Rev. 2017 May;18(5):560–6.
Hamoui N, Kim K, Anthone G, et al. The significance of elevated levels of parathyroid hormone in patients with morbid obesity before and after bariatric surgery. Arch Surg. 2003 Aug;138(8):891–7.
Sinha N, Shieh A, Stein EM, et al. Increased PTH and 1.25(OH)(2)D levels associated with increased markers of bone turnover following bariatric surgery. Obesity (Silver Spring). 2011;19(12):2388–93.
Axelsson KF, Werling M, Eliasson B. Fracture risk after gastric bypass surgery: a retrospective cohort study. J Bone Miner Res. 2018;33(12):2122–31.
Surve A, Zaveri H, Cottam D. Retrograde filling of the afferent limb as a cause of chronic nausea after single anastomosis loop duodenal switch. Surg Obes Relat Dis. 2016;12(4):e39–42.
Zaveri H, Surve A, Cottam D, et al. Stomach intestinal pylorus sparing surgery (SIPS) with laparoscopic fundoplication (LF): a new approach to gastroesophageal reflux disease (GERD) in the setting of morbid obesity. Springerplus. 2015;4:596.
Genco A, Soricelli E, Casella G, et al. Gastroesophageal reflux disease and Barrett's esophagus after laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication. Surg Obes Relat Dis. 2017;13(4):568–74.
Ali M, El Chaar M, Ghiassi S, et al. American Society for Metabolic and Bariatric Surgery updated position statement on sleeve gastrectomy as a bariatric procedure. Surg Obes Relat Dis. 2017;13(10):1652–7.
Acknowledgments
Nicholas Paquette Ph.D. (Medtronic) provided medical writing assistance under the authors’ direction and based on content and conclusions developed by the authors. Sylvain Anselme (Medtronic) provided statistical analysis. Amit Surve, M.D. (Bariatric Medicine Institute, UT) revised the manuscript.
Funding
The study was funded by Medtronic (Mansfield, MA).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of Human and Animal Rights
I certify that the manuscript did not involve the use of animal or human subjects.
Conflict of Interest
Daniel Cottam reports personal fees and other from Medtronic and GI Windows, outside the submitted work. Mitchell Roslin discloses financial relationships with Johnson and Johnson, and Valentx. Dana Portenier discloses financial relationships with Gore, Intuitive, and Teleflex. The remaining authors have no commercial associations that might be a conflict of interest in relation to this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cottam, D., Roslin, M., Enochs, P. et al. Single Anastomosis Duodenal Switch: 1-Year Outcomes. OBES SURG 30, 1506–1514 (2020). https://doi.org/10.1007/s11695-019-04352-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-04352-y