
Abstract
Background
Obesity surgery is the most effective treatment for morbid obesity and the fastest growing area in surgery. Laparoscopic Roux-en-Y gastric bypass (LRYGB) is the gold standard procedure in many countries. Optimization of the treatment process is important in order to keep the morbidity rate down and cost of treatment as low as possible.
Methods
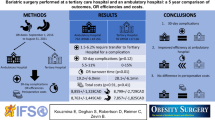
In September 2005, we established a bariatric surgery program. Until December 2010, 2,000 patients underwent LRYGB. Clinical pathways were established, with focus on safety, fast-track methodology and training of surgeons. Time recordings from all parts of the treatment, as well as clinical outcome, were prospectively registered.
Results
Time consumption for the total procedure in the operating theater was reduced from 102 to 54 min (P < 0.001). With only 11 min turnover between patients, the total time for one patient has been reduced to 65 min, enabling us to perform six operations in a single operating theater during ordinary daytime. Early complication rate was 2.8%, and mean hospital stay was 2.3 days. We were able to double the patients treated in 2010 compared to 2007 with only 10% increase in staff. Three surgeons were trained during the period into fully qualified senior bariatric surgeons.
Conclusions
Multimodal evidence-based care within the fast-track methodology and routine time recordings was successful in order to increase the production volumes and reduce costs, without compromising the safety or quality for the patients. This kind of approach may be transferred to other types of standardized surgery.



Similar content being viewed by others


Reference
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2008. Obes Surg. 2009;19(12):1605–11.
Anselmino M, Bammer T, Fernandez Cebrian JM, et al. Cost-effectiveness and budget impact of obesity surgery in patients with type 2 diabetes in three European countries (II). Obes Surg. 2009;19(11):1542–9.
Mullen DM, Marr TJ. Longitudinal cost experience for gastric bypass patients. Surg Obes Relat Dis. 2010;6(3):243–8.
Powers KA, Rehrig ST, Jones DB. Financial impact of obesity and bariatric surgery. Med Clin North Am. 2007;91(3):321–38. ix.
Keating CL, Dixon JB, Moodie ML, et al. Cost-effectiveness of surgically induced weight loss for the management of type 2 diabetes: modeled lifetime analysis. Diabetes Care. 2009;32(4):567–74.
Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248(2):189–98.
Birkmeyer JD, Dimick JB, Staiger DO. Operative mortality and procedure volume as predictors of subsequent hospital performance. Ann Surg. 2006;243(3):411–7.
Main DS, Henderson WG, Pratte K, et al. Relationship of processes and structures of care in general surgery to postoperative outcomes: a descriptive analysis. J Am Coll Surg. 2007;204(6):1157–65.
Lublin M, Lyass S, Lahmann B, et al. Leveling the learning curve for laparoscopic bariatric surgery. Surg Endosc. 2005;19(6):845–8.
Chowdhury MM, Dagash H, Pierro A. A systematic review of the impact of volume of surgery and specialization on patient outcome. Br J Surg. 2007;94(2):145–61.
Lemmens L, van Zelm R, Borel RI, et al. Clinical and organizational content of clinical pathways for digestive surgery: a systematic review. Dig Surg. 2009;26(2):91–9.
Ali MR, Tichansky DS, Kothari SN, et al. Validation that a 1-year fellowship in minimally invasive and bariatric surgery can eliminate the learning curve for laparoscopic gastric bypass. Surg Endosc. 2010;24(1):138–44.
Shikora SA, Kim JJ, Tarnoff ME, et al. Laparoscopic Roux-en-Y gastric bypass: results and learning curve of a high-volume academic program. Arch Surg. 2005;140(4):362–7.
Sommer T, Larsen JF, Raundahl U. Eliminating learning curve-related morbidity in fast track laparoscopic Roux-en-Y gastric bypass. J Laparoendosc Adv Surg Tech A. 2011;21(4):307–12.
Ballantyne GH, Ewing D, Capella RF, et al. The learning curve measured by operating times for laparoscopic and open gastric bypass: roles of surgeon's experience, institutional experience, body mass index and fellowship training. Obes Surg. 2005;15(2):172–82.
Fried M, Hainer V, Basdevant A, et al. Interdisciplinary European guidelines on surgery of severe obesity. Obes Facts. 2008;1(1):52–9.
Leifsson BG, Gislason HG. Laparoscopic Roux-en-Y gastric bypass with 2-metre long biliopancreatic limb for morbid obesity: technique and experience with the first 150 patients. Obes Surg. 2005;15(1):35–42.
Bergland A, Gislason H, Raeder J. Fast-track surgery for bariatric laparoscopic gastric bypass with focus on anaesthesia and peri-operative care. Experience with 500 cases. Acta Anaesthesiol Scand. 2008;52(10):1394–9.
Birkmeyer NJ, Dimick JB, Share D, et al. Hospital complication rates with bariatric surgery in Michigan. JAMA. 2010;304(4):435–42.
Dillemans B, Sakran N, Van CS, et al. Standardization of the fully stapled laparoscopic Roux-en-Y gastric bypass for obesity reduces early immediate postoperative morbidity and mortality: a single center study on 2606 patients. Obes Surg. 2009;19(10):1355–64.
Agaba EA, Shamseddeen H, Gentles CV, et al. Laparoscopic vs open gastric bypass in the management of morbid obesity: a 7-year retrospective study of 1,364 patients from a single center. Obes Surg. 2008;18(11):1359–63.
Conflict of Interest
All contributing authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jacobsen, H.J., Bergland, A., Raeder, J. et al. High-Volume Bariatric Surgery in a Single Center: Safety, Quality, Cost-Efficacy and Teaching Aspects in 2,000 Consecutive Cases. OBES SURG 22, 158–166 (2012). https://doi.org/10.1007/s11695-011-0557-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0557-0