
Abstract
Background
Morbid obesity is associated with different gastrointestinal alterations and diseases. Surgically induced weight loss has become the best treatment for morbidly obese patients. Roux-en-Y gastric bypass is the most common procedure performed worldwide. Concerns regarding difficulties in further evaluation of stomach remnant for early detection of gastric cancer, however, have emphasized the routine use of preoperative upper endoscopy, even in asymptomatic patients, to detect upper gastrointestinal abnormalities. The main outcome of this study was to identify the most common preoperative endoscopic findings.
Methods
Data was collected from a prospective database and medical records of patients with available endoscopic reports, who underwent Roux-en-Y gastric bypass from February 1999 to June 2006. Logistic regression analysis was performed to detect preoperative clinical variables that might be associated with abnormal endoscopy.
Results
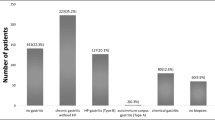
Six hundred twenty-six patients were identified. Four hundred fifty-two (72%) were female; age and body mass index were 38.5 ± 11.3 years and 42 ± 6.5 kg/m2, respectively. Abnormalities were found in 288 (46%) patients. The age of patients with abnormal and normal endoscopy was 40 ± 11 and 36.8 ± 11 years, respectively (p < 0.001). The most common findings were gastritis 21% (n = 132), esophagitis 16% (n = 100), and hiatal hernia 10.7% (n = 67). Duodenitis has a frequency of 7.8% (n = 49), gastric ulcers of 2.7%(n = 17), duodenal ulcers of 2.6% (n = 16), gastric polyps of 1.3% (n = 8), Barrett’s esophagus of 0.16% (n = 1), and gastric cancer of 0.16% (n = 1). Age was the only clinical variable associated to abnormal endoscopy (odds ratio = 1.03; 95% confidence interval, 1.02–1.05).
Conclusions
Routine preoperative endoscopy detects different abnormalities which need specific approach prior to surgery. Preoperative endoscopy should be performed to all patients prior to surgery.
Similar content being viewed by others


References
Koppman JS, Poggi L, Szomstein S, et al. Esophageal motility disorders in the morbidly obese population. Surg Endosc 2007;21:761–4.
Renshaw AA, Rabaza JR, Gonzalez AM, et al. Helicobacter pylori infection in patients undergoing gastric bypass surgery for morbid obesity. Obes Surg 2001;11:281–3.
Hong D, Khajanchee YS, Pereira N, et al. Manometric abnormalities and gastroesophageal reflux disease in the morbidly obese. Obes Surg 2004;14:744–9.
Suter M, Dorta G, Giusti V, et al. Gastro-esophageal reflux and esophageal motility disorders in morbidly obese patients. Obes Surg 2004;14:959–66.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37.
Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg 2004;14:1157–64.
Kuga R, Safatle-Ribeiro AV, Faintuch J, et al. Endoscopic findings in the excluded stomach after Roux-en-y gastric bypass surgery. Arch Surg 2007;142:942–6.
Trincado MT, del Olmo JC, Garcia Castano J, et al. Gastric pouch carcinoma after gastric bypass for morbid obesity. Obes Surg 2005;15:1215–7.
Babor R, Booth M. Adenocarcinoma of the gastric pouch 26 years after loop gastric bypass. Obes Surg 2006;16:935–8.
Zirak C, Lemaitre J, Lebrun E, et al. Adenocarcinoma of the pouch after silastic ring vertical gastroplasty. Obes Surg 2002;12:693–4.
Corsini DA, Simoneti CA, Moreira G, et al. Cancer in the excluded stomach 4 years after gastric bypass. Obes Surg 2006;16:932–4.
Jain PK, Ray B, Royston CM. Carcinoma in the gastric pouch years after vertical banded gastroplasty. Obes Surg 2003;13:136–7.
Khitin L, Roses RE, Birkett DH. Cancer in the gastric remnant after gastric bypass: a case report. Curr Surg 2003;60:521–3.
Escalona A, Guzman S, Ibanez L, et al. Gastric cancer after Roux-en-y gastric bypass. Obes Surg 2005;15:423–7.
Harper JL, Beech D, Tichansky DS, et al. Cancer in the bypassed stomach presenting early after gastric bypass. Obes Surg 2007;17:1268–71.
Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med 2001;345:784–9.
Nih Conference. Gastrointestinal surgery for severe obesity. Consensus development conference panel. Ann Intern Med 1991;115:956–61.
Carrasco F, Klaassen J, Papapietro K, et al. A proposal of guidelines for surgical management of obesity. Rev Med Chil 2005;133:699–706.
Azagury D, Dumonceau JM, Morel P, et al. Preoperative work-up in asymptomatic patients undergoing Roux-en-y gastric bypass: is endoscopy mandatory? Obes Surg 2006;16:1304–11.
Sharaf RN, Weinshel EH, Bini EJ, et al. Endoscopy plays an important preoperative role in bariatric surgery. Obes Surg 2004;14:1367–72.
Madan AK, Speck KE, Hiler ML. Routine preoperative upper endoscopy for laparoscopic gastric bypass: is it necessary? Am Surg 2004;70:684–6.
Correa P. A human model of gastric carcinogenesis. Cancer Res 1988;48:3554–60.
You WC, Blot WJ, Li JY, et al. Precancerous gastric lesions in a population at high risk of stomach cancer. Cancer Res 1993;53:1317–21.
Sasajima K, Kawachi T, Matsukura N, et al. Intestinal metaplasia and adenocarcinoma induced in the stomach of rats by n-propyl-n′-nitro-n-nitrosoguanidine. J Cancer Res Clin Oncol 1979;94:201–6.
Zeni TM, Frantzides CT, Mahr C, et al. Value of preoperative upper endoscopy in patients undergoing laparoscopic gastric bypass. Obes Surg 2006;16:142–6.
Seva-Pereira G, Trombeta VL. Early gastric cancer found at preoperative assessment for bariatric surgery. Obes Surg 2006;16:1109–11.
Boru C, Silecchia G, Pecchia A, et al. Prevalence of cancer in Italian obese patients referred for bariatric surgery. Obes Surg 2005;15:1171–6.
Acknowledgements
Dr. Muñoz scholarship is funded by MECESUP and Faculty of Medicine, Pontificia Universidad Católica de Chile. Authors want to thanks Dr. Osvaldo Llanos for its comments and revision of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Muñoz, R., Ibáñez, L., Salinas, J. et al. Importance of Routine Preoperative Upper GI Endoscopy: Why All Patients Should Be Evaluated?. OBES SURG 19, 427–431 (2009). https://doi.org/10.1007/s11695-008-9673-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9673-x