
Abstract
Background
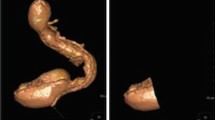
Sleeve gastrectomy (SG), which, thus far, is showing good resolution of comorbidities and good weight loss, shows increasing popularity among bariatric surgeons. The aim of this study was to evaluate clinical outcome and the gastric emptying of solid foods, 24 months after SG.
Methods
Fourteen morbidly obese patients, four males and ten females, median age 41 years (range 29–65), median body mass index (BMI) 49.46 kg/m2 (range 41.14–55.63), who underwent SG for weight loss, were studied prospectively. Nine patients underwent gastric emptying studies, using radioisotopic technique before, 6 months and 24 months after the operation. The remaining five patients underwent gastric emptying studies, 6 months and 24 months after the operation.
Results
A significant reduction in patients’ weight and BMI was evident at 6, 12 and 24 months postoperatively. In the nine patients who underwent gastric emptying studies pre-, 6 and 24 months postoperatively, the T-lag phase duration significantly decreased, following the SG, from 17.30 (range 15.50–20.90) min, to 12.50 (range 9.20–18.00) min at 6 months and 12.16 (range 10.90–20.00) min at 24 months postoperatively (P < 0.05). The gastric emptying half time (T1/2) accelerated significantly postoperatively from 86.50 (range 77.50–104.60) min, to 62.50 (range 46.30–80.00) min at 6 months and 60.80 (range 54.80–100.00) min at 24 months after SG (P < 0.05). The percentage of gastric emptying (%GE) increased significantly postoperatively, from 52 (range 43–58) % to 72 (range 57–97) % at 6 months and 74 (range 45–82) % at 24 months, following SG (P < 0.05). No differences in gastric emptying were observed, when values at 24 months were compared to those at 6 months postoperatively. When the whole group of 14 patients was studied, there were also no significant changes in T-lag, T1/2 and %GE between 6 and 24 months postoperatively.
Conclusions
Our study indicates the constant effect of SG in the acceleration of gastric emptying of solids, which occurs faster, not only in short but also in long-term postoperatively. Such effects on gastric motility, in combination with the reported alterations in gut hormones, may explain how this ‘food limiting’ operation results in weight loss.

Similar content being viewed by others


References
World Health Organization fact sheet No 311, September 2006. www.who.int/topics/obesity
Deitel M. The obesity epidemic. Obes Surg. 2006;16:377–8.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–37.
Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547–59.
Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240:416–23.
Melissas J. IFSO guidelines for safety, quality, and excellence in bariatric surgery. Obes Surg. 2008;18:497–500.
Baltasar A, Serra C, Pérez N, et al. Laparoscopic sleeve gastrectomy: a multi-purpose bariatric operation. Obes Surg. 2005;15:1124–8.
Deitel M, Crosby RD, Gagner M. The first international consensus summit for sleeve gastrectomy (SG), New York City, October 25–27, 2007. Obes Surg. 2008;18:487–96.
Almogy G, Crookes PF, Anthone GJ. Longitudinal gastrectomy as a treatment for the high-risk super-obese patient. Obes Surg. 2004;14:492–7.
Regan JP, Inabnet WB, Gagner M, et al. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg. 2003;13:861–4.
Tucker ON, Szomstein S, Rosenthal RJ. Indications for sleeve gastrectomy as a primary procedure for weight loss in the morbidly obese. J Gastrointest Surg. 2008;12:662–7.
Näslund E, Hellström PM, Kral JG. The gut and food intake: an update for surgeons. J Gastrointest Surg. 2001;5:556–67.
Wynne K, Stanley S, Bloom S. The gut and regulation of body weight. J Clin Endocrinol Metab. 2004;89:2576–82.
Melissas J, Koukouraki S, Askoxylakis J, et al. Sleeve gastrectomy: a restrictive procedure? Obes Surg. 2007;17:57–62.
Nasreddine L, Hwalla N, Sibai A, et al. Food consumption patterns in an adult population in Beirut, Lebanon. Public Health Nutr. 2006;9:194–203.
Deitel M, Gawdat K, Melissas J. Reporting weight loss 2007. Obes Surg. 2007;17:565–68.
Ziessman HA, Fahey FH, Atkins FB, et al. Standardization and quantification of radionuclide solid gastric-emptying studies. J Nucl Med. 2004;45:760–4.
Tosetti C, Corinaldesi R, Stanghellini V, et al. Gastric emptying of solids in morbid obesity. Int J Obes Relat Metab Disord. 1996;20:200–5.
Verdich C, Madsen JL, Toubro S, et al. Effect of obesity and major weight reduction on gastric emptying. Int J Obes Relat Metab Disord. 2000;24:899–905.
Jackson SJ, Leahy FE, McGowan AA, et al. Delayed gastric emptying in the obese: an assessment using the non-invasive (13)C-octanoic acid breath test. Diabetes Obes Metab. 2004;6:264–70.
Mistiaen W, Vaneerdeweg W, Blockx P, et al. Gastric emptying rate measurement after vertical banded gastroplasty. Obes Surg. 2000;10:245–9.
Nocca D, Krawczykowsky D, Bomans B, et al. A prospective multicenter study of 163 sleeve gastrectomies: results at 1 and 2 years. Obes Surg. 2008;18:560–5.
Melissas J, Christodoulakis M, Schoretsanitis G, et al. Obesity-associated disorders before and after weight reduction by vertical banded gastroplasty in morbidly vs super obese individuals. Obes Surg. 2001;11:475–81.
Carmichael AR, Johnston D, Barker MC, et al. Gastric emptying after a new, more physiological anti-obesity operation: the Magenstrasse and Mill procedure. Eur J Nucl Med. 2001;28:1379–83.
Bended N, Livshitz G, Mindlin L, et al. Gastric emptying half-time following silastic ring vertical gastroplasty: a scintigraphic study. Obes Surg. 1996;6:459–62.
Weiner RA, Weiner S, Pomhoff I, et al. Laparoscopic sleeve gastrectomy—influence of sleeve size and resected gastric volume. Obes Surg. 2007;17:1297–305.
Kojima M, Hosoda H, Date Y, et al. Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature. 1999;402:656–60.
Lee HM, Wang G, Englander EW, et al. Ghrelin, a new gastrointestinal endocrine peptide that stimulates insulin secretion: enteric distribution, ontogeny, influence of endocrine and dietary manipulations. Endocrinology. 2002;143:185–90.
Langer FB, Reza Hoda MA, Bohdjalian A, et al. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg. 2005;15:1024–9.
Kotidis EV, Koliakos G, Papavramidis TS, et al. The effect of biliopancreatic diversion with pylorus-preserving sleeve gastrectomy and duodenal switch on fasting serum ghrelin, leptin and adiponectin levels: is there a hormonal contribution to the weight-reducing effect of this procedure? Obes Surg. 2006;16:554–9.
Morinigo R, Moizé V, Musri M, et al. Glucagon-like peptide-1, peptide YY, hunger and satiety after gastric bypass surgery in morbidly obese subjects. J Clin Endocrinol Metab. 2006;91:1735–40.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Melissas, J., Daskalakis, M., Koukouraki, S. et al. Sleeve Gastrectomy—A “Food Limiting” Operation. OBES SURG 18, 1251–1256 (2008). https://doi.org/10.1007/s11695-008-9634-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9634-4