
Background
Obstructive sleep apnea is a common condition in patients undergoing bariatric surgery.The aim of this study was to determine the clinical outcome of a cohort of morbidly obese patients with documented sleep apnea who underwent laparoscopic Roux-en- Y gastric bypass (LRYGBP).
Methods
56 morbidly obese patients with documented sleep apnea by polysomnography underwent LRYGBP. There were 36 females with mean age 46 years and mean BMI 49 kg/m2.The Epworth sleepiness scale (ESS) scores and the number of patients requiring the use of continuous positive airway pressure (CPAP) therapy were recorded preoperatively and at 3-month intervals.
Results
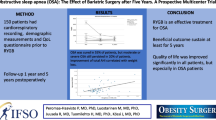
The mean length of sleep apnea condition was 44 ±55 months. Preoperative polysomnography scores were classified as severe in 50% of patients, moderate in 30%, and mild in 20%. 29 of 56 (52%) patients required CPAP therapy preoperatively. The mean excess body weight loss was 73 ±3% at 12 months. The mean ESS score decreased from 13.7 preoperatively to 5.3 at 1 month postoperatively (P<0.05) and maintained below the threshold level (<7) for the entire 12 months of follow-up. Of the 29 patients requiring preoperative CPAP, only 4 (14%) patients required CPAP at 3 months postoperatively and none required CPAP at 9 months.
Conclusions
Weight loss associated with LRYGBP significantly improves the symptoms of sleep apnea and is effective in discontinuation in the clinical use of CPAP therapy. Improvement of obstructive sleep apnea symptoms occur as early as 1 month postoperatively.
Similar content being viewed by others

References
O’Keeffe T, Patterson EJ. Evidence supporting routine polysomnography before bariatric surgery. Obes Surg 2004; 14: 23–6.
Sidana J, Aronow WS, Ravipati G et al. Prevalence of moderate or severe left ventricular diastolic dysfunction in obese persons with obstructive sleep apnea. Cardiology 2005; 104: 107–9.
Ballantyne GH, Svahn J, Capella RF et al. Predictors of prolonged hospital stay following open and laparoscopic gastric bypass for morbid obesity: body mass index, length of surgery, sleep apnea, asthma, and the metabolic syndrome. Obes Surg 2004; 14: 1042–50.
Yaggi HK, Concato J, Kernan WN et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 10; 353: 2034–41.
Valencia-Flores M, Orea A, Herrera M et al. Effect of bariatric surgery on obstructive sleep apnea and hypopnea syndrome, electrocardiogram, and pulmonary arterial pressure. Obes Surg 2004; 14: 755–62.
Buchwald H, Avidor Y, Braunwald E et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004; 292: 1724–37.
Rasheid S, Banasiak M, Gallagher SF et al. Gastric bypass is an effective treatment for obstructive sleep apnea in patients with clinically significant obesity. Obes Surg 2003; 13: 58–61.
Sugerman HJ, Fairman RP, Sood RK et al. Long-term effects of gastric surgery for treating respiratory insufficiency of obesity. Am J Clin Nutr 1992; 55 (Suppl 2): 597S–601S.
Lankford DA, Proctor CD, Richard R. Continuous positive airway pressure (CPAP) changes in bariatric surgery patients undergoing rapid weight loss. Obes Surg 2005; 15: 336–41.
Haines KL, Nelson LG, Gonzalez R et al. Objective evidence that bariatric surgery improves obesity-related obstructive sleep apnea. Surgery 2007; 141: 354–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Varela, J.E., Hinojosa, M.W. & Nguyen, N.T. Resolution of Obstructive Sleep Apnea after Laparoscopic Gastric Bypass. OBES SURG 17, 1279–1282 (2007). https://doi.org/10.1007/s11695-007-9228-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9228-6