
Background
Laparoscopic adjustable gastric banding (LAGB) is a safe and effective treatment for morbid obesity that is well suited to outpatient surgery. Super-obese patients (BMI ≥50) are often viewed as higher risk patients, with their surgical procedures limited to hospital operating-rooms. We report our experience performing LAGB for super-obese patients in a freestanding ambulatory surgery center and describe the program elements that make this feasible and safe.
Methods
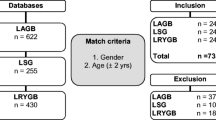
Database records containing 1,780 consecutive patients from program inception (November 2002 to November 2006) were searched for patients with a BMI >49.9 undergoing an outpatient LAGB and reviewed to identify complications.
Results
320 super-obese patients underwent an outpatient LAGB.Mean preoperative weight was 155.2 kg (range 112.3–220.5 kg), and mean BMI was 55.4 kg/m2 (range 50.0–71.1 kg/m2). 53 patients (16.6%) had BMI >60. There were no deaths, significant cardiopulmonary complications, significant intraoperative bleeding, conversion to open laparotomy, or hospital admissions. 3 patients (0.1%) developed gastric edema causing transient obstruction, and 1 developed a delayed colon perforation from electrocautery incurred during adhesiolysis. No complication arose or was more difficult to manage as a result of the procedure being done on an outpatient basis.
Conclusions
Outpatient LAGB can be safely performed in super-obese patients with a complication rate similar to lower BMI patients. Patient selection and preoperative preparation are essential to achieve excellent outcomes. The decision to offer an outpatient LAGB should rest on the overall physiological condition rather than BMI or weight alone.
Similar content being viewed by others

References
Watkins BM, Montgomery KF, Ahroni JA et al. Adjustable gastric banding in an ambulatory surgery center. Obes Surg 2005; 15: 1045–9.
Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Draft Statement. Obes Surg 1991; 1: 257–66.
Dixon JB, McPhail T, O’Brien PE. Minimal reporting requirements for weight loss: Current methods not ideal. Obes Surg 2005; 15:1034–9; discussion 1041–4.
Dixon JB, Schachter LM, O’Brien PE. Predicting sleep apnea and excessive day sleepiness in the severely obese. Chest 2003; 123: 1134–41.
Ren CJ, Fielding GA. Laparoscopic adjustable gastric banding: Surgical technique. J Laparoendosc Adv Surg Tech A 2003; 13: 257–63.
Watkins BM, Montgomery KF, Ahroni JA. Laparoscopic adjustable gastric banding: Early experience in 400 consecutive patients in the USA. Obes Surg 2005; 15: 82–7.
Recommendations for facilities performing bariatric surgery. Bull Am Coll Surg 2000; 85: 20–3.
Dolan K, Finch R, Fielding G. Laparoscopic gastric banding and crural repair in the obese patient with a hiatal hernia. Obes Surg 2003; 13: 772–5.
Fris RJ. Preoperative low energy diet diminishes liver size. Obes Surg 2004; 14: 1165–70.
Colles SL, Dixon JB, Marks P et al. Preoperative weight loss with a very-low-energy diet: Quantitation of changes in liver and abdominal fat by serial imaging. Am J Clin Nutr 2006; 84: 304–11.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Montgomery, K.F., Watkins, B.M., Ahroni, J.H. et al. Outpatient Laparoscopic Adjustable Gastric Banding in Super-obese Patients. OBES SURG 17, 711–716 (2007). https://doi.org/10.1007/s11695-007-9149-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9149-4