
Abstract
Summary
We compared the utility of the current Romanian guidelines that recommend treatment in women with a T-score ≤−2.5 SD with a FRAX-based intervention threshold equivalent to women with a prior fragility fracture. Whereas the FRAX-based intervention threshold identified women at high fracture probability, the T-score threshold was less sensitive and decreased markedly with age.
Purpose
FRAX® algorithm has been calibrated for Romania, but guidance is needed on how to apply fracture probabilities to clinical practice.
Methods
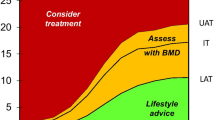
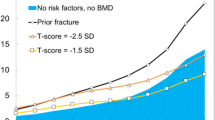
The age-specific 10-year probabilities of a major osteoporotic fracture were calculated at two potential intervention thresholds. The first comprised the age-specific fracture probabilities associated with a femoral neck T-score of −2.5 SD, in line with Romanian guidelines. The second approach determined age-specific fracture probabilities that were equivalent to a woman with a prior fragility fracture, without bone mineral density (BMD). The parsimonious use of BMD was additionally explored by the computation of upper and lower assessment thresholds for BMD testing.
Results
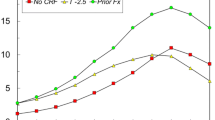
When a BMD T-score ≤−2.5 SD was used as an intervention threshold, FRAX probabilities in women aged 50 years were twofold higher than in women of the same age with an average BMD. The increase in risk associated with the BMD threshold decreased progressively with age such that, at the age of 80 years or more, a T-score of −2.5 SD was protective. The 10-year probability of a major osteoporotic fracture by age, equivalent to women with a previous fracture, rose from 5.3 % at the age of 50 years to 13 % at the age of 80 years and identified women at increased risk at all ages.
Conclusion
Intervention thresholds based on BMD alone do not effectively target women at high fracture risk, particularly in the elderly. In contrast, intervention thresholds based on fracture probabilities equivalent to a “fracture threshold” targets women at high fracture risk irrespective of age.


Similar content being viewed by others
References
Poole KE, Compston JE (2006) Osteoporosis and its management. BMJ 333(7581):1251–1256
Kanis JA, Oden A, Johnell O, Jonsson B, de Laet C, Dawson A (2001) The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int 12(5):417–427
Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR (1991) Which fractures are associated with low appendicular bone mass in elderly women? The Study of Osteoporotic Fractures Research Group. Ann Intern Med 115(11):837–842
Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J et al (2013) Osteoporosis in the European Union: Medical Management, Epidemiology and Economic Burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos (in press)
World Health Organization (2007) Assessment of osteoporosis at the primary health care level. WHO, Geneva
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312(7041):1254–1259
Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P et al (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20(7):1185–1194
Kanis JA, Johnell O (2005) Requirements for DXA for the management of osteoporosis in Europe. Osteoporos Int 16(3):229–238
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19(4):385–397
Grigorie D, Sucaliuc A, Johansson H, Kanis JA, McCloskey E (2013) Incidence of hip fracture in Romania and the development of a Romanian FRAX model. Calcif Tissue Int 92(5):429–436. doi:10.1007/s00223-013-9697-7
Lekamwasam S, Adachi JD, Agnusdei D, Bilezikian J, Boonen S, Borgstrom F et al (2012) A framework for the development of guidelines for the management of glucocorticoid-induced osteoporosis. Osteoporos Int 23(9):2257–2276
Kanis JA, McCloskey EV, Johansson H, Cooper C, Rizzoli R, Reginster JY (2013) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 24(1):23–57
Kanis JA, McCloskey E, Johansson H, Oden A, Leslie WD (2012) FRAX((R)) with and without bone mineral density. Calcif Tissue Int 90(1):1–13
Kanis JA, Oden A, Johnell O, Johansson H, De Laet C, Brown J et al (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18(8):1033–1046
Johansson H, Oden A, Johnell O, Jonsson B, de Laet C, Oglesby A et al (2004) Optimization of BMD measurements to identify high risk groups for treatment—a test analysis. J Bone Miner Res 19(6):906–913
Leslie WD, Majumdar SR, Lix LM, Johansson H, Oden A, McCloskey E et al (2012) High fracture probability with FRAX usually indicates densitometric osteoporosis: implications for clinical practice. Osteoporos Int 23(1):391–397
Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A (2008) Case finding for the management of osteoporosis with FRAX–assessment and intervention thresholds for the UK. Osteoporos Int 19(10):1395–1408
Kanis JA, Johnell O, Oden A, Jonsson B, De Laet C, Dawson A (2000) Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 27(5):585–590
Johansson H, Kanis JA, Oden A, Johnell O, McCloskey E (2009) BMD, clinical risk factors, and their combination for hip fracture prevention. Osteoporos Int 20(10):1675–1682
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Grigorie, D., Sucaliuc, A., Johansson, H. et al. FRAX-based intervention and assessment thresholds for osteoporosis in Romania. Arch Osteoporos 8, 164 (2013). https://doi.org/10.1007/s11657-013-0164-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-013-0164-x