
Abstract
Background
Medical care at the end of life is often expensive and ineffective.
Objective
To explore associations between primary care and hospital utilization at the end of life.
Design
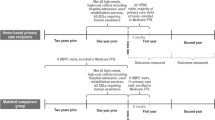
Retrospective analysis of Medicare data. We measured hospital utilization during the final 6 months of life and the number of primary care physician visits in the 12 preceding months. Multivariate cluster analysis adjusted for the effects of demographics, comorbidities, and geography in end-of-life healthcare utilization.
Subjects
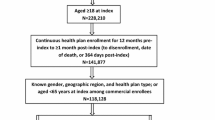
National random sample of 78,356 Medicare beneficiaries aged 66+ who died in 2001. Non-whites were over-sampled. All subjects with complete Medicare data for 18 months prior to death were retained, except for those in the End Stage Renal Disease program.
Measurements
Hospital days, costs, in-hospital death, and presence of two types of preventable hospital admissions (Ambulatory Care Sensitive Conditions) during the final 6 months of life.
Results
Sample characteristics: 38% had 0 primary care visits; 22%, 1–2; 19%, 3–5; 10%, 6–8; and 11%, 9+ visits. More primary care visits in the preceding year were associated with fewer hospital days at end of life (15.3 days for those with no primary care visits vs. 13.4 for those with ≥9 visits, P < 0.001), lower costs ($24,400 vs. $23,400, P < 0.05), less in-hospital death (44% vs. 40%, P < 0.01), and fewer preventable hospitalizations for those with congestive heart failure (adjusted odds ratio, aOR = 0.82, P < 0.001) and chronic obstructive pulmonary disease (aOR = 0.81, P = 0.02).
Conclusions
Primary care visits in the preceding year are associated with less, and less costly, end-of-life hospital utilization. Increased primary care access for Medicare beneficiaries may decrease costs and improve quality at the end of life.
Similar content being viewed by others

REFERENCES
Hogan C, Lunney J, Gabel J, Lynn J. Medicare beneficiaries’ costs of care in the last year of life. Health Aff. 2001;204188–95.
Edwards C, DeHaven T. War betweeen the generations: federal spending on the elderly set to explode. In: C. Institute, eds. Policy Analysis. Washington D.C.; 2003: 1–22.
Approaching Death: Improving Care at the End of Life. Washington D.C.: National Academy Press; 1997.
Ezekiel EJ. Cost savings at the end of life: What do the data show? JAMA. 1996;275241907–14.
Campbell D, Lynn J, Louis T, Shugarman L. Medicare program expenditures associated with hospice use. Ann Intern Med. 2004;140:269–77.
Degenholtz HB, Rhee Y, Arnold RM. Brief communication: the relationship between having a living will and dying in place. Ann Intern Med. 2004;1412113–7.
SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients: the study to understand prognoses and preferences for outcomes and risks of treatments. JAMA. 1995;274:1591–8.
Patrick D, Curtis R, Engelberg R, Nielsen E, McCown E. Measuring and improving the quality of dying and death. Ann Intern Med. 2003;1392410–5.
Burge F, Lawson B, Johnston G. Family physician continuity of care and emergency department use in end-of-life cancer care. Med Care. 2003;418992–1001.
Burge F, Lawson B, Johnston G, Cummings I. Primary care continuity and location of death for those with cancer. J Palliat Med. 2003;66911–8.
De Maeseneer JM, De Prins L, Gosset C, Heyerick J. Provider continuity in family medicine: does it make a difference for total health care costs? Ann Fam Med. 2003;13144–8.
Gill JM, Mainous AG 3rd. The role of provider continuity in preventing hospitalizations. Arch Fam Med. 1998;74352–7.
Saultz JW, Albedaiwi W. Interpersonal continuity of care and patient satisfaction: a critical review. Ann Fam Med. 2004;25445–51.
Cabana MD, Jee SH. Does continuity of care improve patient outcomes? J Fam Pract. 2004;5312974–80.
Ash AS, Ellis RP, Pope GC, et al. Using diagnoses to describe populations and predict costs. Health Care Financ Rev. 2000;2137–28.
Burns RB, McCarthy EP, Freund KM, et al. Black women receive less mammography even with similar use of primary care. Ann Intern Med. 1996;125:173–82.
Keating NL, Landrum MB, Ayanian JZ, et al. The association of ambulatory care with breast cancer stage at diagnosis among Medicare beneficiaries. J Gen Intern Med. 2005;20:38–44.
Ricketts TC, Randolph R, Howard HA, Pathman D, Carey T. Hospitalization rates as indicators of access to primary care. Health & Place. 2001;7127–38.
Agency for Healthcare Research and Quality. Refinement of the HCUP Quality Indicators. 2001 Summary, Technical Review Number 4. Available at: http://www.qualityindicators.ahrq.gov/downloads/technical/qi_technical_summary.pdf. Accessed March 12, 2008.
Norman Levinsky M, Wei Yu P, Arlene Ash P, et al. Influence of age on medicare expenditures and medical care in the last year of life. JAMA. 2001;286111349–55.
Valentin A, Jordan B, Lang T, Hiesmayr M, Metnitz PGH. Gender-related differences in intensive care: A multiple-center cohort study of therapeutic interventions and outcome in critically ill patients. Crit Care Med. 2003;3171901–7.
Degenholtz HB, Thomas SB, Miller MJ. Race and the intensive care unit: disparities and preferences for end-of-life care. Crit Care Med. 2003;315 SupplS373–8.
Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162202269–76.
Ash AS, Posner MA, Speckman J, Franco S, Yacht AC, Bramwell L. Using claims data to examine mortality trends following hospitalization for heart attack in Medicare. Health Serv Res. 2003;3851253–62.
Pritchard RS, Fisher ES, Teno JM, et al. Influence of patient preferences and local health system characteristics on the place of death. SUPPORT investigators. Study to understand prognoses and preferences for risks and outcomes of treatment. J Am Geriatr Soc. 1998;46101242–50.
Baicker K, Chandra A, Skinner JS, Wennberg JE. Who you are and where you live: how race and geography affect the treatment of medicare beneficiaries. Health Aff. 2004;(Suppl Web Exclusive):VAR33–44.
Wennberg JE, Fisher ES, Stukel TA, Skinner JS, Sharp SM, Bronner KK. Use of hospitals, physician visits, and hospice care during last six months of life among cohorts loyal to highly respected hospitals in the United States. BMJ. 2004;3287440607.
Emanuel E, Emanuel L. The economics of dying–the illusion of cost savings at the end of life. N Engl J Med. 1994;3308540–4.
Shugarman LR, Campbell DE, Bird CE, Gabel J, Louis TA, Lynn J. Differences in medicare expenditures during the last 3 years of life. J Gen Intern Med. 2004;192127–35.
Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, Part 2. JAMA. 2002;288151909–14.
Grabowski DC, Stewart KA, Broderick SM, et al. Predictors of nursing home hospitalization: a review of the literature. Med Care Res Rev. 2008;6513–39.
Weinberger M, Oddone EZ, Henderson WG. Does increased access to primary care reduce hospital readmissions? Veterans affairs cooperative study group on primary care and hospital readmission. N Engl J Med. 1996;334221441–7.
Bodenheimer T. Primary care–will it survive? N Engl J Med. 2006;3559861–4.
Fisher ES, Wennberg JE, Stukel TA, et al. Associations among hospital capacity, utilization, and mortality of US Medicare beneficiaries, controlling for sociodemographic factors. Health Serv Res. 34(6):1351–62.
Zhao Y, Ash AS, Ellis RP, Slaughter JP. Disease burden profiles: an emerging tool for managing managed care. Health Care Manage Sci. 2002;53211–9.
Kronman A, Hanchate A, Ash AS. Improving risk adjustment for illness burden. J Gen Intern Med. 2007;22(s1). Abstract.
Health Care Financing Review: Medicare and Medicaid Statistical Supplement. US Dept. of Health and Human Services, Centers for Medicare and Medicaid Services, Office of Research, Development and Information, 2003.
Statement for the Record for Senate HELP Committee Hearing on Addressing Healthcare Workforce Issues for the Future (12-Feb-08): A Report from the American College of Physicians; 2008. Available at: http://www.acponline.org/advocacy/where_we_stand/workforce/pc_workforce.pdf Accessed March 12, 2008.
Acknowledgements
This work was presented at the AcademyHealth Annual Research Meeting in Orlando, FL, on 4 June 2006 and received the Mack Lipkin Sr. Associate Member Award for Outstanding Scientific Presentation at the National Meeting for the Society of General Internal Medicine in Los Angeles, CA, on 26 April 2006. The authors thank Drs. Jim Burgess and John Pagliaro for their support with manuscript preparation, and Jenn Fonda for support with computer programming. Dr. Kronman is supported by a Mentored Clinical Scientist Development Program Award (Building Interdisciplinary Careers in Women’s Health Research) from the National Institutes of Health (K12 HD04344, Karen Freund, Principal Investigator). Dr. Kronman was supported by an Institutional National Research Service Award from the National Institutes of Health (T32 HP 10028, Rob Friedman, Principal Investigator) when this research was performed.
Conflict of Interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kronman, A.C., Ash, A.S., Freund, K.M. et al. Can Primary Care Visits Reduce Hospital Utilization Among Medicare Beneficiaries at the End of Life?. J GEN INTERN MED 23, 1330–1335 (2008). https://doi.org/10.1007/s11606-008-0638-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-008-0638-5