
Abstract
Purpose
This study has aimed to evaluate the effects of surgery on physical activity (PA), quality of life (QoL), and disease-specific health status, by analyzing the differences between sphincter-preserving surgery (low anterior resection (LAR)) and abdominoperineal resection (APR) among rectal cancer survivors.
Methods
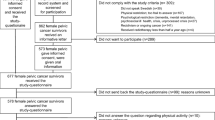
Individuals who were diagnosed with rectal cancer and who underwent an APR or a LAR between 2000 and 2009 were included. The different questionnaires on QoL, disease-specific health status, and physical activity began their surveys in 2010. Differences in QoL, health status, and physical activity were analyzed between the APR group and the LAR group.
Results
The study included 905 rectal cancer survivors (LAR, 632; APR, 273). Besides a higher rate of radiotherapy treatment in the APR group (94% vs. 75%, p < 0.001), there were no differences in clinical characteristics or in comorbid conditions between the LAR group and APR group. No significant differences were found in PA level between the patients who had undergone an APR vs. a LAR. Regarding QoL, APR patients did report a worse physical (p = 0.009) and role functioning (p = 0.03), as well as a worse body image (p = 0.001), compared to patients who had undergone a LAR. However, they reported fewer constipation (p = 0.02) and gastrointestinal problems (p = 0.009). Finally, compared to patients who had undergone a LAR with a permanent ostomy, APR patients reported a better body image (p = 0.048) and less stoma-related problems (p = 0.001).
Conclusions
This study showed no differences in PA level among the patients who had undergone an APR versus a LAR. With respect to their QoL, their physical and role functioning seemed to be worse in the APR patients. However, these differences in outcomes resolved when comparing the APR group with patients after a LAR with a permanent ostomy.

Similar content being viewed by others


Abbreviations
- APR:
-
Abdominoperineal resection
- ECR:
-
Eindhoven Cancer Registry
- EORTC QLQ-C30:
-
European Organization for Research and Treatment of Cancer Quality of Life Questionnaire
- QoL:
-
Quality of life
- LAR:
-
Low anterior resection
- LARS:
-
Low anterior resection syndrome
- LMM:
-
Linear mixed models
- PROFILES:
-
Patient Reported Outcomes Following Initial Treatment and Long Term Evaluations of Survivorship
- PA:
-
Physical activity
References
Weitz, J., et al., Colorectal cancer. Lancet, 2005. 365(9454): p. 153–65.
Sprangers, M.A., et al., Quality of life in colorectal cancer. Stoma vs. nonstoma patients. Dis Colon Rectum, 1995. 38(4): p. 361–9.
Emmertsen, K.J. and S. Laurberg, Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg, 2012. 255(5): p. 922–8.
Engel, J., et al., Quality of life in rectal cancer patients: a four-year prospective study. Ann Surg, 2003. 238(2): p. 203–13.
Traa, M.J., et al., Sexual (dys)function and the quality of sexual life in patients with colorectal cancer: a systematic review. Ann Oncol, 2012. 23(1): p. 19–27.
Traa, M.J., et al., Measuring the health-related quality of life and sexual functioning of patients with rectal cancer: does type of treatment matter? Int J Cancer, 2014. 134(4): p. 979–87.
Konanz, J., et al., Quality of life of patients after low anterior, intersphincteric, and abdominoperineal resection for rectal cancer--a matched-pair analysis. Int J Colorectal Dis, 2013. 28(5): p. 679–88.
Hassan, I. and R.R. Cima, Quality of life after rectal resection and multimodality therapy. J Surg Oncol, 2007. 96(8): p. 684–92.
Mols, F., et al., Chemotherapy-induced neuropathy and its association with quality of life among 2- to 11-year colorectal cancer survivors: results from the population-based PROFILES registry. J Clin Oncol, 2013. 31(21): p. 2699–707.
Janssen-Heijnen MLG, L. W., Van de Poll-Franse LV, Coebergh JWW, Results of 50 years cancer registry in the south of the Netherlands. Vol. 1955-2004 (in Dutch). 2005, Eindhoven: Eindhoven Cancer Regist.
Sangha, O., et al., The Self-Administered Comorbidity Questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum, 2003. 49(2): p. 156–63.
Aaronson, N.K., et al., The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst, 1993. 85(5): p. 365–76.
Fayers PM, A. N., Bjordal K, Groenvold M, Crran D, Bottomley A, O.b.o.t. EORTC QoL Group, The EORTC QLQ-C30 Scoring Manual. 3 ed. 2001, Brussels: EORTC Publications.
Sprangers, M.A., A. te Velde, and N.K. Aaronson, The construction and testing of the EORTC colorectal cancer-specific quality of life questionnaire module (QLQ-CR38). European Organization for Research and Treatment of Cancer Study Group on Quality of Life. Eur J Cancer, 1999. 35(2): p. 238–47.
Pols, M.A., et al., Estimation of reproducibility and relative validity of the questions included in the EPIC Physical Activity Questionnaire. Int J Epidemiol, 1997. 26 Suppl 1: p. S181–9.
Ainsworth, B.E., et al., Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc, 1993. 25(1): p. 71–80.
Ainsworth, B.E., et al., Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc, 2000. 32(9 Suppl): p. S498–504.
Cocks, K., et al., Evidence-based guidelines for determination of sample size and interpretation of the European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30. J Clin Oncol, 2011. 29(1): p. 89–96.
Norman, G.R., J.A. Sloan, and K.W. Wyrwich, Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care, 2003. 41(5): p. 582–92.
Kornmann, M., D. Henne-Bruns, and F. Porzsolt, Neoadjuvant treatment of rectal carcinoma: assessment of health care services by physicians and lay persons. J Clin Oncol, 2008. 26(30): p. 4866–8.
Orsini, R.G., et al., Quality of life of older rectal cancer patients is not impaired by a permanent stoma. Eur J Surg Oncol, 2013. 39(2): p. 164–70.
Hamaker, M.E., et al., Long-term changes in physical capacity after colorectal cancer treatment. J Geriatr Oncol, 2015. 6(2): p. 153–64.
Bretagnol, F., et al., Long-term functional results after sphincter-saving resection for rectal cancer. Gastroenterol Clin Biol, 2004. 28(2): p. 155–9.
Bruheim, K., et al., Sexual function in males after radiotherapy for rectal cancer. Int J Radiat Oncol Biol Phys, 2010. 76(4): p. 1012–7.
Bruheim, K., et al., Sexual function in females after radiotherapy for rectal cancer. Acta Oncol, 2010. 49(6): p. 826–32.
Havenga, K., et al., Male and female sexual and urinary function after total mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. J Am Coll Surg, 1996. 182(6): p. 495–502.
Hendren, S.K., et al., Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer. Ann Surg, 2005. 242(2): p. 212–23.
Acknowledgements
The researchers would like to thank all of the patients and their doctors for their participation in this study. A special thanks goes to Dr. M. van Bommel, who was willing to function as an independent advisor and to answer the questions of the patients. In addition, the researchers want to thank the following hospitals for their cooperation: Amphia Hospital, Breda; the Bernhoven Hospitals in Veghel and Oss; Catharina Hospital, Eindhoven; Elkerliek Hospital, Helmond; Jeroen Bosch Hospital, ‘s-Hertogenbosch; the Máxima Medical Centers in Eindhoven and Veldhoven; Sint Anna Hospital, Geldrop; Elisabeth – TweeSteden Hospital, Tilburg; and the VieCury Hospitals in Venlo and Venray..
Financial Support
The data collection for this study was funded by a VENI Grant (no. 451-10-041) from the Netherlands Organization for Scientific Research (The Hague, The Netherlands) awarded to Floortje Mols, together with a Medium Investment Grant from the Netherlands Organization for Scientific Research (The Hague, The Netherlands, NWO No. 480-08-009).
Dr. Dounya Schoormans (No. UVT2013-5893) was supported by a Social Psychology Fellowship from the Dutch Cancer Society, Amsterdam, The Netherlands.
These funding agencies had no further role in the study’s design; in the collection, the analyses and the interpretation of the data; in the writing of the paper; and in the decision to submit this paper for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by a local Dutch Certified Medical Ethics Committee. All of the patients gave their informed consent. The manuscript has been prepared in accordance with the style of the journal and all of the authors have approved its contents. This manuscript is not being considered for publication elsewhere and the findings in this manuscript have not been previously published.
Conflict of Interest
The authors declare that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Koëter, T., Bonhof, C.S., Schoormans, D. et al. Long-term Outcomes After Surgery Involving the Pelvic Floor in Rectal Cancer: Physical Activity, Quality of Life, and Health Status. J Gastrointest Surg 23, 808–817 (2019). https://doi.org/10.1007/s11605-018-4014-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-4014-4