
Abstract
Introduction
Tumors of the neck of the pancreas may involve the superior mesenteric and portal veins as well as the termination of the splenic vein. This presents a difficult problem since the pancreas cannot be transected through the neck as is standard in a Whipple procedure. Here, we present our method of resecting such tumors, which we term “Whipple at the Splenic Artery (WATSA)”.
Methods
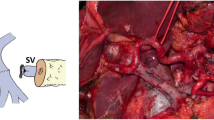
The superior mesenteric and portal veins are isolated below and above the pancreas, respectively. The pancreas and splenic vein are divided just to the right of the point that the splenic artery contacts the superior border of the pancreas. This plane of transection is approximately 2 cm to the left of the pancreatic neck and away from the tumor. The superior mesenteric artery is cleared from the left side of the patient. With the specimen remaining attached only by the superior mesenteric and portal veins, these structures are clamped and divided. Reconstruction is performed with or without a superficial femoral vein graft. The splenic vein is not reconstructed.
Results
Ten cases have been performed to date without mortality. We have previously shown that the pattern of venous collateral development following occlusion of the termination of the splenic vein in the manner described is not similar to that of cases of sinistral (left sided) portal hypertension.
Discussion
Whipple at the splenic artery (WATSA) is a safe method for resection of tumors of the neck of the pancreas with vein involvement. It should be performed in high-volume pancreatic surgery centers.







Similar content being viewed by others

References
Fortner JG. Technique of regional subtotal and total pancreatectomy. Am J Surg 1985;150:593-600.
Fuhrman GM, Leach SD, Staley CA, et al. Rationale for en bloc vein resection in the treatment of pancreatic adenocarcinoma adherent to the superior mesenteric-portal vein confluence. Pancreatic Tumor Study Group. Ann Surg 1996;223:154-62.
Tamura K, Sumi S, Koike M, Yano S, Nagami H, Nio Y. A splenic-inferior mesenteric venous anastomosis prevents gastric congestion following pylorus preserving pancreatoduodenectomy with extensive portal vein resection for cancer of the head of the pancreas. International Surgery 1997;82:155-9.
Leach SD, Lee JE, Charnsangavej C, et al. Survival following pancreaticoduodenectomy with resection of the superior mesenteric-portal vein confluence for adenocarcinoma of the pancreatic head. Brit J Surg 1998;85:611-7.
Ishikawa O, Ohigashi H, Sasaki Y, et al. Intraoperative cytodiagnosis for detecting a minute invasion of the portal vein during pancreatoduodenectomy for adenocarcinoma of the pancreatic head. Am J Surg 1998;175:477-81.
Launois B, Stasik C, Bardaxoglou E, et al. Who benefits from portal vein resection during pancreaticoduodenectomy or pancreatic cancer? World J Surg 1999;23:926-9.
Howard TJ, Villanustre N, Moore SA, et al. Efficacy of venous reconstruction in patients with adenocarcinoma of the pancreatic head. J Gastrointest Surg 2003;7:1089-95.
Yoshimi F, Asato Y, Tanaka R, et al. Reconstruction of the portal vein and the splenic vein in pancreaticoduodenectomy for pancreatic cancer. Hepatogastroent 2003;50:856-60.
Poon RT, Fan ST, Lo CM, et al. Pancreaticoduodenectomy with en bloc portal vein resection for pancreatic carcinoma with suspected portal vein involvement. World J Surg 2004;28:602-8.
Muller SA, Hartel M, Mehrabi A, et al. Vascular resection in pancreatic cancer surgery: survival determinants. J Gastrointest Surg 2009;13:784-92.
Misuta K, Shimada H, Miura Y, et al. The role of splenomesenteric vein anastomosis after division of the splenic vein in pancreatoduodenectomy. J Gastrointest Surg 2005;9:245-53.
Smoot RL, Christein JD, Farnell MB. Durability of portal venous reconstruction following resection during pancreaticoduodenectomy. J Gastrointest Surg 2006;10:1371-5.
Riediger H, Makowiec F, Fischer E, Adam U, Hopt UT. Postoperative morbidity and long-term survival after pancreaticoduodenectomy with superior mesenterico-portal vein resection. J Gastrointest Surg 2006;10:1106-15.
Yekebas EF, Bogoevski D, Cataldegirmen G, et al. En bloc vascular resection for locally advanced pancreatic malignancies infiltrating major blood vessels: perioperative outcome and long-term survival in 136 patients. Ann Surg 2008;247:300-9.
Martin RC, 2nd, Scoggins CR, Egnatashvili V, Staley CA, McMasters KM, Kooby DA. Arterial and venous resection for pancreatic adenocarcinoma: operative and long-term outcomes. Arch Surg 2009;144:154-9.
Toomey P, Hernandez J, Morton C, et al. Resection of portovenous structures to obtain microscopically negative margins during pancreaticoduodenectomy for pancreatic adenocarcinoma is worthwhile. Am Surg 2009;75:804-9.
Kaneoka Y, Yamaguchi A, Isogai M. Portal or superior mesenteric vein resection for pancreatic head adenocarcinoma: prognostic value of the length of venous resection. Surgery 2009;145:417-25.
Stauffer JA, Dougherty MK, Kim GP, Nguyen JH. Interposition graft with polytetrafluoroethylene for mesenteric and portal vein reconstruction after pancreaticoduodenectomy. Brit J Surg 2009;96:247-52.
Porembka M, Linehan D, Hawkins W, Strasberg S. Radiologic and intraoperative detection of need for vein resection in patients with adenocarcinoma of the head of the pancreas. HPB 2011;13:633-42.
Tashiro S, Uchino R, Hiraoka T, et al. Surgical indication and significance of portal vein resection in biliary and pancreatic cancer. Surgery 1991;109:481-7.
Strasberg SM, Bhalla S, Sanchez LA, Linehan DCJGS. Pattern of Venous Collateral Development After Splenic Vein Occlusion in an Extended Whipple Procedure: Comparison with Collateral Vein Pattern in Cases of Sinistral Portal Hypertension. J Gastrointest Surg 2011;15:2070–2079
Strasberg SM, Drebin JA, Mokadam NA et al. Prospective Trial of a Blood Supply-Based Technique of Pancreaticojejunostomy: Effect on Anastomotic Failure in the Whipple Procedure. J Am Coll Surg 2002; 194:56-58.
Pedrazzoli S, DiCarlo V, Dionigi R, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Ann Surg 1998;228:508-17.
Yeo CJ, Cameron JL, Lillemoe KD, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg 2002;236:355-66.
Farnell MB, Pearson RK, Sarr MG, et al. A prospective randomized trial comparing standard pancreatoduodenectomy with pancreatoduodenectomy with extended lymphadenectomy in resectable pancreatic head adenocarcinoma. Surgery 2005;138:618-28.
Michalski CW, Kleeff J, Wente MN, Diener MK, Buchler MW, Friess H. Systematic review and meta-analysis of standard and extended lymphadenectomy in pancreaticoduodenectomy for pancreatic cancer. [Review] [54 refs]. Brit J Surg 2007;94:265-73.
Acknowledgments
Supported by a grant from the Turpin Family HPB Surgery Division Fund.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Strasberg, S.M., Sanchez, L.A., Hawkins, W.G. et al. Resection of Tumors of the Neck of the Pancreas with Venous Invasion: the “Whipple at the Splenic Artery (WATSA)” Procedure. J Gastrointest Surg 16, 1048–1054 (2012). https://doi.org/10.1007/s11605-012-1841-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-012-1841-6