
Abstract
Introduction
The recently published 7th edition of the American Joint Committee on Cancer (AJCC) TNM staging criteria for gastric adenocarcinoma contains important revisions to T and N classifications, as well as overall stage grouping. Our goal was to validate the new staging system using a cancer registry.
Methods
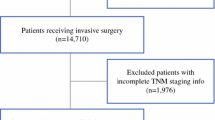
Retrospective review of gastric cancer patients from Surveillance, Epidemiology, and End Results (SEER) registry data (2004–2007). Patients were staged according to both 6th and 7th edition criteria, and 3-year disease-specific survival was compared.
Results
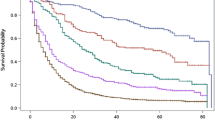
Thirteen thousand five hundred forty-seven patients with gastric adenocarcinoma were identified with complete staging information. When using 7th edition criteria, there was an increase in the number of patients classified as stage III (23% vs. 13%), and a decrease in patients classified as stage IV (47% vs. 53%). Statistically significant differences in 3-year disease-specific survival were observed for all T and N categories and re-staging the same population according to the 7th edition criteria improved survival discrimination. Multivariate analysis revealed statistically significant differences in survival and linear progression of hazard ratios for each stage grouping.
Conclusions
The 7th edition AJCC staging criteria for gastric adenocarcinoma demonstrate better survival discrimination and risk stratification than previous criteria.


Similar content being viewed by others

References
Garcia M, Jemal A, Ward EM, et al. Global cancer facts and figures 2007. Atlanta: American Cancer Society, 2007.
Greene, FL, Page, DL, Fleming, ID, et al (Eds.). AJCC Cancer staging manual, 6th edition. New York: Springer, 2002.
Ahn HS, Lee HJ, Hahn S, Kim WH, Lee KU, Sano T, Edge SB, Yang HK. “Evaluation of the 7th American Joint Committee on Cancer/International Union Against Cancer Classification of gastric adenocarcinoma in comparison with the 6th classification.” Cancer 116, no. 24 (2010): 5592–8.
Chae S, Lee A, Lee JH. “The effectiveness of the new (7th) UICC N classification in the prognosis evaluation of gastric cancer patients: a comparative study between the 5th/6th and 7th UICC N classification.” Gastric Cancer, 2011: (in press).
Jung H, Lee HH, Song KY, Jeon HM, Park CH. “Validation of the 7th edition of the American joint committee on cancer TNM staging system for gastric cancer.” Cancer, 2011: (in press).
Wang W, Sun XW, Li CF, Lv L, Li YF, Chen YB, Xu DZ, Kesari R, Huang CY, Li W, Zhan YQ, Zhou ZW. “Comparison of the 6th and 7th Editions of the UICC TNM Staging System for Gastric Cancer: Results of a Chinese Single-Institution Study of 1,503 Patients.” Ann Surg Oncol, 2011: (in press).
Leung WK, Wu MS, Kakugawa Y, Kim JJ, Yeoh KG, Goh KL, Wu KC, Wu DC, Sollano J, Kachintorn U, Gotoda T, Lin JT, You WC, Ng EK, Sung JJ. “Screening for gastric cancer in Asia: current evidence and practice.” Lancet Oncol 9, no. 3 (2008): 279–87.
Havener, L. “Standards for cancer registries volume III: standards for completeness, quality, analysis, and management of data. North American Association of Central Cancer Registries.” 2004.
National Cancer Institute. http://seer.cancer.gov/index.html . (accessed October 2010).
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (Eds.). AJCC cancer staging manual, 7th edition. New York: Springer, 2010.
Lu Y, Liu C, Zhang R, Li H, Lu P, Jin F, Xu H, Wang S, Chen J. “Prognostic significance of subclassification of pT2 gastric cancer: a retrospective study of 847 patients.” Surg Oncol 17, no. 4 (2008): 317–22.
Nitti D, Marchet A, Mocellin S, Rossi GM, Ambrosi A, Mencarelli R. “Prognostic value of subclassification of T2 tumours in patients with gastric cancer.” Br J Surg 96, no. 4 (2009): 398–404.
Park Do J, Kong SH, Lee HJ, Kim WH, Yang HK, Lee KU, Choe KJ. “Subclassification of pT2 gastric adenocarcinoma according to depth of invasion (pT2a vs pT2b) and lymph node status (pN).” Surgery 141, no. 6 (2007): 757–63.
Aurello P, D’Angelo F, Rossi S, Bellagamba R, Cicchini C, Nigri G, Ercolani G, De Angelis R, Ramacciato G. “Classification of lymph node metastases from gastric cancer: comparison between N-site and N-number systems. Our experience and review of the literature.” Am Surg 73, no. 4 (2007): 359–66.
Ichikura T, Tomimatsu S, Uefuji K, Kimura M, Uchida T, Morita D, Mochizuki H. “Evaluation of the New American Joint Committee on Cancer/International Union against cancer classification of lymph node metastasis from gastric carcinoma in comparison with the Japanese classification.” Cancer 86, no. 4 (1999): 553–8.
Kodera Y, Yamamura Y, Shimizu Y, Torii A, Hirai T, Yasui K, Morimoto T, Kato T, Kito T. “Lymph node status assessment for gastric carcinoma: is the number of metastatic lymph nodes really practical as a parameter for N categories in the TNM classification? Tumor Node Metastasis.” J Surg Oncol 69, no. 1 (1998): 15–20.
Roder JD, Böttcher K, Busch R, Wittekind C, Hermanek P, Siewert JR. “Classification of regional lymph node metastasis from gastric carcinoma. German Gastric Cancer Study Group.” Cancer 82, no. 4 (1998): 621–31.
Asoglu O, Karanlik H, Parlak M, Kecer M, Muslumanoglu M, Igci A, Ozmen V, Gulluoglu M, Kapran Y. “Metastatic lymph node ratio is an independent prognostic factor in gastric cancer.” Hepatogastroenterology 56, no. 91–92 (2009): 908–13.
Chua YJ, Cunningham D. “The UK NCRI MAGIC trial of perioperative chemotherapy in resectable gastric cancer: implications for clinical practice.” Ann Surg Oncol 14, no. 10 (2007): 2687–90.
Strong VE, Song KY, Park CH, Jacks LM, Gonen M, Shah M, Coit DG, Brennan MF. “Comparison of gastric cancer survival following R0 resection in the United States and Korea using an internationally validated nomogram.” Ann Surg 251, no. 4 (2010): 640–6.
Hundahl SA, Phillips JL, Menck HR. “The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: Fifth Edition American Joint Committee on Cancer staging, proximal disease, and the ”different disease“ hypothesis.” Cancer 88, no. 4 (2000): 921–32.
Kattan MW, Karpeh MS, Mazumdar M, Brennan MF. “Postoperative nomogram for disease-specific survival after an R0 resection for gastric carcinoma.” J Clin Oncol 21, no. 19 (2003): 3647–50.
Washington, K. “7th edition of the AJCC cancer staging manual: stomach.” Ann Surg Oncol 17, no. 12 (2010): 3077–9.
Acknowledgments
None.
Conflicts of interest
The authors declare that they have no conflicts of interest
Author information
Authors and Affiliations
Corresponding author
Additional information
Discussant
Dr. Han-Kwang Yang (Seoul, Korea): I am glad to hear that your conclusion is favorable with the new 7th staging system, in which our institute’s survival data were used as one of the principal reference data. You used 3DFS in this analysis. GASTRIC group presented that 3DFS can replace 5ys in gastric cancer at ASCO meeting 2009. Now, Japanese Gastric Cancer Association adopted this 7th edition, too.
But there are a few problems on the 7th edition as you mentioned.
1. Esophago Gastric junction tumor invading esophagus was classified to Esophageal cancer, which is not appropriate according to our analysis.
2. N3a vs. N3b should be further investigated.
For the next revision of TNM staging system, International Gastric Cancer Association just launched a TFT which will include database from all over the world.
When I look at the general characteristics table of your SEER database, I have a few questions on the general practice of surgery for gastric cancer in the USA.
Question#1. Average or median number LN examined per patient for each stage?
Question#2. In the type of surgery, what does it mean “local excision” (39%) in the era of 2004–2007?
I am concerned on this description of surgery. If I assume proximal cancers are more operated in the specialized centers, this might be related to the independently significantly poor prognosis of distal location compared with proximal location. We know that radiation can not compensate inadequate surgery. This could explain why the survival for each stage of SEER database is worse than those from Asia.
Question #3. Who dissects the LN of the specimen? If surgeon does specimen dissection, it will improve the pathologic evaluation of LN status.
Closing Discussant
Drs. Lee J. McGhan & Nabil Wasif: Thank you Dr. Yang for reviewing our manuscript, and for your insightful comments and questions. I would like to first address the point you raised about classification of proximal gastric tumors within 5 cm of the GE junction involving the GE junction as esophageal cancers in the AJCC classification. We are limited in our analysis of this dataset by being unable to classify tumors by location beyond being “proximal” in location. It is also possible that many of these tumors are treated as esophageal cancers and underwent neo-adjuvant chemoradiation with subsequent downstaging which may have resulted in the improved survival seen in our analysis.
In answer to your first question, the median lymph node counts for stage I–III patients were 10, 11, and 15, respectively. Although most patients in our series did not have >15 lymph nodes excised, we re-analyzed our data to look at patients who did have >15 lymph nodes examined and noticed the same improvement in survival discrimination with the 7th AJCC classification as compared with the 6th.
Secondly, the term “local excision” as used in our study encompasses all techniques used to remove the tumor that do not involve surgical resection. This includes techniques such as polypectomy and endoscopic mucosal resection or EMR.
Finally, lymph nodes are typically found in the specimen by the pathology assistant and then processed and examined by the pathologist, as is the case at our institution. The surgeons are usually not involved. Studies on the subject have shown an improvement in lymph node counts when a standardized processing protocol is applied in the pathology laboratory and we aim to achieve this at our institution; this may need to applied at the national level. The involvement of surgeons in labeling lymph node stations may indeed also be useful.
Rights and permissions
About this article
Cite this article
McGhan, L.J., Pockaj, B.A., Gray, R.J. et al. Validation of the Updated 7th Edition AJCC TNM Staging Criteria for Gastric Adenocarcinoma. J Gastrointest Surg 16, 53–61 (2012). https://doi.org/10.1007/s11605-011-1707-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-011-1707-3