
Abstract
Background
The outcomes of complex major surgery in the elderly are being scrutinized because of the demands on surgical services by an aging population and the concern whether such endeavors are justified. Pancreatoduodenectomy (PD) for pancreatic adenocarcinoma presents special challenges because of the high morbidity of the procedure, dismal prognosis of the disease, and the increasing incidence of pancreatic cancer with age.
Methods
All patients who underwent PD for pancreatic adenocarcinoma from 1981 to 2007 were analyzed for perioperative outcomes, tumor-related parameters, use of adjuvant therapy, and long-term survival. Specifically those aged ≥80 years were compared with a control group aged ≤80 years. Continuous variables are displayed as median and interquartile range (IQR); log-rank test and Cox’s proportional hazards were used to determine survival and effect of age as an independent marker against other covariates.
Results
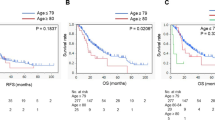
Fifty-three patients aged ≥80 years underwent PD. Twenty-six (51%) developed complications, including delayed gastric emptying (nine, 17%), pancreatic leak (six, 11%), and postoperative bleeding (five, 9%). There was one in-hospital death (2%). The hospital stay was 13.5 days (IQR 9–19). Forty-one (79%) patients were discharged home; of the 11 (21%) patients who went to an outside health care facility (pancreatic leak/drains and feeding issues—five, delayed gastric emptying/nutritional—four, no home support—one), one died in a nursing home at 5 months while the other ten patients returned to their previous abode (median 4 weeks). The median disease-free and overall survivals were 11.8 (IQR 7.8–18.4) and 13.5 months (IQR 12–21.3). Compared to the non-octogenarians (n = 567), the older population had more poor risk patients with respect to ASA status (P < 0.0004), stayed longer as in-patients (P < 0.04), were more likely to develop complications (P < 0.001), and were less likely to receive adjuvant therapy (P < 0.0001). There was no difference in long-term disease-free or overall survival (log-rank P < 0.30 and P < 0.14), and age did not appear to be an independent marker of prognosis when analyzed (Cox’s proportional hazards P < 0.26; chi-square, 1.25).
Conclusions
In experienced institutions, PD for ductal adenocarcinoma is a viable option in the ambulatory octogenarian population who are deemed operative candidates for a PD. The trade off is a greater complication rate and the prospect of discharge (one in five) to a chronic care facility. The majority, however, can be discharged home with a reasonable functional status, and those discharged to temporary health care rehabilitation facilities are likely to make a recovery over a few weeks.

Similar content being viewed by others

References
United States Census Bureau. 2008 National Population Projections. http://www.census.gov/population/www/projections/.
US Census Bureau. 1990 Census. http://factfinder.census.gov/servlet/DatasetMainPageServlet?_lang=en&_ts=246063658125&_ds_name=DEC_1990_STF1_&_program=.
Crile G, Jr. The advantages of bypass operations over radical pancreatoduodenectomy in the treatment of pancreatic carcinoma. Surg Gynecol Obstet 1970; 130(6):1049–53.
Shapiro TM. Adenocarcinoma of the pancreas: a statistical analysis of biliary bypass vs Whipple resection in good risk patients. Ann Surg 1975; 182(6):715–21.
Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-five consecutive pancreaticoduodenectomies without mortality. Ann Surg 1993; 217(5):430–5; discussion 435–8.
Schnelldorfer T, Ware AL, Sarr MG, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg 2008; 247(3):456–62.
DiCarlo V, Balzano G, Zerbi A, Villa E. Pancreatic cancer resection in elderly patients. Br J Surg 1998; 85(5):607–10.
Fong Y, Blumgart LH, Fortner JG, Brennan MF. Pancreatic or liver resection for malignancy is safe and effective for the elderly. Ann Surg 1995; 222(4):426–34; discussion 434–7.
Brozzetti S, Mazzoni G, Miccini M, et al. Surgical treatment of pancreatic head carcinoma in elderly patients. Arch Surg 2006; 141(2):137–42.
Sohn TA, Yeo CJ, Cameron JL, et al. Should pancreaticoduodenectomy be performed in octogenarians? J Gastrointest Surg 1998; 2(3):207–16.
Spencer MP, Sarr MG, Nagorney DM. Radical pancreatectomy for pancreatic cancer in the elderly. Is it safe and justified? Ann Surg 1990; 212(2):140–3.
Hosking MP, Warner MA, Lobdell CM, et al. Outcomes of surgery in patients 90 years of age and older. Jama 1989; 261(13):1909–15.
Huang JJ, Yeo CJ, Sohn TA, et al. Quality of life and outcomes after pancreaticoduodenectomy. Ann Surg 2000; 231(6):890–8.
Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg 2004; 240(2):293–8.
Hardacre JM, Simo K, McGee MF, et al. Pancreatic resection in octogenarians. J Surg Res 2009; 156(1):129–32.
Makary MA, Winter JM, Cameron JL, et al. Pancreaticoduodenectomy in the very elderly. J Gastrointest Surg 2006; 10(3):347–56.
Tani M, Kawai M, Hirono S, et al. A pancreaticoduodenectomy is acceptable for periampullary tumors in the elderly, even in patients over 80 years of age. J Hepatobiliary Pancreat Surg 2009; 16(5):675–80.
Chen JW, Shyr YM, Su CH, et al. Is pancreaticoduodenectomy justified for septuagenarians and octogenarians? Hepatogastroenterology 2003; 50(53):1661–4.
Scurtu R, Bachellier P, Oussoultzoglou E, et al. Outcome after pancreaticoduodenectomy for cancer in elderly patients. J Gastrointest Surg 2006; 10(6):813–22.
Shaw CM, O'Hanlon DM, McEntee GP. Long-term quality of life following pancreaticoduodenectomy. Hepatogastroenterology 2005; 52(63):927–32.
Nieveen van Dijkum EJ, Kuhlmann KF, Terwee CB, et al. Quality of life after curative or palliative surgical treatment of pancreatic and periampullary carcinoma. Br J Surg 2005; 92(4):471–7.
Nguyen TC, Sohn TA, Cameron JL, et al. Standard vs. radical pancreaticoduodenectomy for periampullary adenocarcinoma: a prospective, randomized trial evaluating quality of life in pancreaticoduodenectomy survivors. J Gastrointest Surg 2003; 7(1):1–9; discussion 9–11.
Schniewind B, Bestmann B, Kurdow R, et al. Bypass surgery versus palliative pancreaticoduodenectomy in patients with advanced ductal adenocarcinoma of the pancreatic head, with an emphasis on quality of life analyses. Ann Surg Oncol 2006; 13(11):1403–11.
Lightner AM, Glasgow RE, Jordan TH, et al. Pancreatic resection in the elderly. J Am Coll Surg 2004; 198(5):697–706.
Finlayson E, Fan Z, Birkmeyer JD. Outcomes in octogenarians undergoing high-risk cancer operation: a national study. J Am Coll Surg 2007; 205(6):729–34.
Yermilov I, Bentrem D, Sekeris E, et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: a population-based appraisal. Ann Surg Oncol 2009; 16(3):554–61.
Lea MS, Stahlgren LH. Is resection appropriate for adenocarcinoma of the pancreas? A cost-benefit analysis. Am J Surg 1987; 154(6):651–4.
Vickers SM, Kerby JD, Smoot TM, et al. Economics of pancreatoduodenectomy in the elderly. Surgery 1996; 120(4):620–5; discussion 625–6.
Topal B, Peeters G, Vandeweyer H, et al. Hospital cost-categories of pancreaticoduodenectomy. Acta Chir Belg 2007; 107(4):373–7.
Rosemurgy AS, Bloomston M, Serafini FM, et al. Frequency with which surgeons undertake pancreaticoduodenectomy determines length of stay, hospital charges, and in-hospital mortality. J Gastrointest Surg 2001; 5(1):21–6.
Ho V, Aloia T. Hospital volume, surgeon volume, and patient costs for cancer surgery. Med Care 2008; 46(7):718–25.
Pratt WB, Gangavati A, Agarwal K, et al. Establishing standards of quality for elderly patients undergoing pancreatic resection. Arch Surg 2009; 144(10):950–6.
Bassi C, Dervenis C, Butturini G, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138(1):8–13.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khan, S., Sclabas, G., Lombardo, K.R. et al. Pancreatoduodenectomy for Ductal Adenocarcinoma in the Very Elderly; Is It Safe and Justified?. J Gastrointest Surg 14, 1826–1831 (2010). https://doi.org/10.1007/s11605-010-1294-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-010-1294-8