
Abstract
Purpose
The purpose of the study was to determine the utility of routine contrast enema prior to ileostomy closure and its impact on patient management in patients with a low pelvic anastomosis.
Material and Methods
Two hundred eleven patients had a temporary loop ileostomy constructed to protect a low colorectal or coloanal anastomosis following low anterior resection for cancer (57%) or other disease (12%) or to protect an ileal pouch–anal anastomosis following restorative proctocolectomy (31%). All patients were evaluated by physical examination, proctoscopy, and water-soluble contrast enema prior to ileostomy closure. Imaging results were correlated with the clinical situation to determine the effects on patient management.
Results
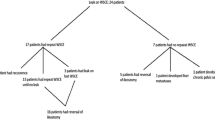
The mean time from ileostomy creation to closure was 15.6 weeks. Overall, 203 patients (96%) had an uncomplicated course. Eight patients (4%) developed an anastomotic leak, seven of which were diagnosed clinically and confirmed radiographically before planned ileostomy closure. Resolution of the leak was confirmed by follow-up contrast enema. One patient, whose pouchogram revealed a normal anastomosis, clinically developed a leak after ileostomy closure. It is important to note that routine contrast enema examination did not reveal an anastomotic leak or stricture that was not already suspected clinically.
Conclusions
All patients who developed an anastomotic leak in this study were diagnosed clinically, and the diagnosis was confirmed by selective use of radiographic tests. Routine contrast enema evaluation of low pelvic anastomoses before loop ileostomy closure did not provide any additional information that changed patient management. The utility of this routine practice should be questioned.
Similar content being viewed by others


References
Fujita S, Teramoto T, Watanabe M, Kodaira S, Kitajima M. Anastomotic leakage after colorectal cancer surgery: a risk factor for recurrence and poor prognosis. Jpn J Clin Oncol 1993;23:299–302.
Ogunbiyi OA, Korsgen S, Keighley MR. Pouch salvage. Long-term outcome. Dis Colon Rectum 1997;40:548–552.
Karanjia ND, Corder AP, Bearn P, Heald RJ. Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg 1994;81:1224–1226.
Dehni N, Schlegel RD, Cunningham C, Guiguet M, Tiret E, Parc R. Influence of a defunctioning stoma on leakage rates after low colorectal anastomosis and colonic J pouch-anal anastomosis. Br J Surg 1998;85:1114–1117.
Hallbook O, Sjodahl R. Anastomotic leakage and functional outcome after anterior resection of the rectum. Br J Surg 1996;83:60–62.
Karanjia ND, Corder AP, Holdsworth PJ, Heald RJ. Risk of peritonitis and fatal septicaemia and the need to defunction the low anastomosis. Br J Surg 1991;78:196–198.
Remzi FH, Fazio VW, Gorgun E, et al. The outcome after restorative proctocolectomy with or without defunctioning ileostomy. Dis Colon Rectum 2006;49:470–477.
Vignali A, Fazio VW, Lavery IC, et al. Factors associated with the occurrence of leaks in stapled rectal anastomoses: a review of 1,014 patients. J Am Coll Surg 1997;185:105–113.
Fazio VW, Ziv Y, Church JM, et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 1995;222:120–127.
Konishi T, Watanabe T, Kishimoto J, et al. Risk factors for anastomotic leakage after surgery for colorectal cancer: results of prospective surveillance. J Am Coll Surg 2006;202:439–444.
Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 1998;85:355–358.
Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351:1731–1740.
Brown JJ, Balfe DM, Heiken JP, et al. Ileal J pouch: radiologic evaluation in patients with and without postoperative infectious complications. Radiology 1990;174:115–120.
Thoeni RF, Fell SC, Engelstad B, Schrock TB. Ileoanal pouches: comparison of CT, scintigraphy, and contrast enemas for diagnosing postsurgical complications. Am J Roentgenol 1990;154:73–88.
da Silva GM, Wexner SD, Gurland B, et al. Is routine pouchogram prior to ileostomy closure in colonic J-pouch really necessary? Colorectal Dis 2004;6:117–120.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kalady, M.F., Mantyh, C.R., Petrofski, J. et al. Routine Contrast Imaging of Low Pelvic Anastomosis Prior to Closure of Defunctioning Ileostomy: is it Necessary?. J Gastrointest Surg 12, 1227–1231 (2008). https://doi.org/10.1007/s11605-008-0510-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-008-0510-2