
Abstract
Background
Hepatic artery chemoembolization (HACE) is a treatment option in the management of metastatic carcinoid. We reviewed our experience to identify potential factors that influence survival.
Methods
The records of 122 patients with metastatic carcinoid tumor undergoing HACE were reviewed. Log-rank analysis and Cox proportional hazards were applied to identify factors predictive of decreased survival.
Results
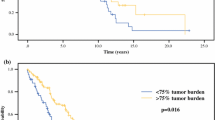
Median follow-up after HACE was 21.5 months. Complications occurred in 23% with periprocedural mortality of 5%. Radiographic tumor regression was seen in 82%, with stabilization of disease in 12%. Median duration of CT response was 19 months. Improvement in symptoms occurred in 92% for median duration of 13 months. HACE resulted in complete normalization of serum pancreastatin in 14%, with greater than 20% reduction in another 66%. Median overall survival was 33.3 months after HACE. Only pancreastatin level ≥5,000 pg/ml was associated with decreased survival by multivariate analysis.
Conclusion
HACE offers symptom palliation and long-term survival in patients with incurable carcinoid metastases. Although safe, it should be approached cautiously in patients with significant tumor burden as evidenced by pancreastatin levels ≥5,000 pg/ml. We do not recommend whole-liver embolization in these patients but prefer a staged approach to each lobe of the liver.


Similar content being viewed by others


References
Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003;97(4):934–959.
Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer 1997;79(4):813–829.
Brown KT, Koh BY, Brody LA, Getrajdman GI, Susman J, Fong Y, Blumgart LH. Particle embolization of hepatic neuroendocrine metastases for control of pain and hormonal symptoms. J Vasc Interv Radiol 1999;10(4):397–403.
Diaco DS, Hajarizadeh H, Mueller CR, Fletcher WS, Pommier RF, Woltering EA. Treatment of metastatic carcinoid tumors using multimodality therapy of octreotide acetate, intra-arterial chemotherapy, and hepatic arterial chemoembolization. Am J Surg 1995;169(5):523–528.
Drougas JG, Anthony LB, Blair TK, Lopez RR, Wright JK, Jr., Chapman WC, Webb L, Mazer M, Meranze S, Pinson CW. Hepatic artery chemoembolization for management of patients with advanced metastatic carcinoid tumors. Am J Surg 1998;175(5):408–412.
Nobin A, Mansson B, Lunderquist A. Evaluation of temporary liver dearterialization and embolization in patients with metastatic carcinoid tumour. Acta Oncol 1989;28(3):419–424.
O’Toole D, Ruszniewski P. Chemoembolization and other ablative therapies for liver metastases of gastrointestinal endocrine tumours. Best Pract Res Clin Gastroenterol 2005;19(4):585–594.
Atwell TD, Charboneau JW, Que FG, Rubin J, Lewis BD, Nagorney DM, Callstrom MR, Farrell MA, Pitot HC, Hobday TJ. Treatment of neuroendocrine cancer metastatic to the liver: the role of ablative techniques. Cardiovasc Interv Radiol 2005;28(4):409–421.
Desai DC, O’Dorisio TM, Schirmer WJ, Jung SS, Khabiri H, Villanueva V, Martin EW. Serum pancreastatin levels predict response to hepatic artery chemoembolization and somatostatin analogue therapy in metastatic neuroendocrine tumors. Regul Pept 2001;96(3):113–117.
Strosberg JR, Choi J, Cantor AB, Kvols LK. Selective hepatic artery embolization for treatment of patients with metastatic carcinoid and pancreatic endocrine tumors. Cancer Control 2006;13(1):72–78.
Gupta S, Johnson MM, Murthy R, Ahrar K, Wallace MJ, Madoff DC, McRae SE, Hicks ME, Rao S, Vauthey JN, Ajani JA, Yao JC. Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 2005;104(8):1590–1602.
Chamberlain RS, Canes D, Brown KT, Saltz L, Jarnagin W, Fong Y, Blumgart LH. Hepatic neuroendocrine metastases: does intervention alter outcomes? J Am Coll Surg 2000;190(4):432–445.
Osborne DA, Zervos EE, Strosberg J, Boe BA, Malafa M, Rosemurgy AS, Yeatman TJ, Carey L, Duhaine L, Kvols LK. Improved outcome with cytoreduction versus embolization for symptomatic hepatic metastases of carcinoid and neuroendocrine tumors. Ann Surg Oncol 2006;13(4):572–581.
Sarmiento JM, Que FG. Hepatic surgery for metastases from neuroendocrine tumors. Surg Oncol Clin N Am 2003;12(1):231–242.
Shebani KO, Souba WW, Finkelstein DM, Stark PC, Elgadi KM, Tanabe KK, Ott MJ. Prognosis and survival in patients with gastrointestinal tract carcinoid tumors. Ann Surg 1999;229(6):815–821; discussion 822–823.
Yao KA, Talamonti MS, Nemcek A, Angelos P, Chrisman H, Skarda J, Benson AB, Rao S, Joehl RJ. Indications and results of liver resection and hepatic chemoembolization for metastatic gastrointestinal neuroendocrine tumors. Surgery 2001;130(4):677–682; discussion 682–685.
Gupta S, Yao JC, Ahrar K, Wallace MJ, Morello FA, Madoff DC, Murthy R, Hicks ME, Ajani JA. Hepatic artery embolization and chemoembolization for treatment of patients with metastatic carcinoid tumors: the M.D. Anderson experience. Cancer J 2003;9(4):261–267.
Boudreaux JP, Putty B, Frey DJ, Woltering E, Anthony L, Daly I, Ramcharan T, Lopera J, Castaneda W. Surgical treatment of advanced-stage carcinoid tumors: lessons learned. Ann Surg 2005;241(6):839–845; discussion 845–6.
Berger DH, Carrasco CH, Hohn DC, Curley SA. Hepatic artery chemoembolization or embolization for primary and metastatic liver tumors: post-treatment management and complications. J Surg Oncol 1995;60(2):116–121.
Ramage JK, Davies AH. Measurement of quality of life in carcinoid/neuroendocrine tumours. Endocr Relat Cancer 2003;10(4):483–486.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van Oosterom AT, Christian MC, Gwyther SG. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000;92(3):205–216.
Calhoun K, Toth-Fejel S, Cheek J, Pommier R. Serum peptide profiles in patients with carcinoid tumors. Am J Surg 2003;186(1):28–31.
Kimura N, Funakoshi A, Aunis D, Tateishi K, Miura W, Nagura H. Immunohistochemical localization of chromostatin and pancreastatin, chromogranin A-derived bioactive peptides, in normal and neoplastic neuroendocrine tissues. Endocr Pathol 1995;6(1):35–43.
Oberg K. The ultimate biochemical diagnosis of gastro-enteropancreatic tumours. Digestion 1996;57 Suppl 1:45–47.
Stridsberg M, Oberg K, Li Q, Engstrom U, Lundqvist G. Measurements of chromogranin A, chromogranin B (secretogranin I), chromogranin C (secretogranin II) and pancreastatin in plasma and urine from patients with carcinoid tumours and endocrine pancreatic tumours. J Endocrinol 1995;144(1):49–59.
Eriksson BK, Larsson EG, Skogseid BM, Lofberg AM, Lorelius LE, Oberg KE. Liver embolizations of patients with malignant neuroendocrine gastrointestinal tumors. Cancer 1998;83(11):2293–2301.
Ruszniewski P, Rougier P, Roche A, Legmann P, Sibert A, Hochlaf S, Ychou M, Mignon M. Hepatic arterial chemoembolization in patients with liver metastases of endocrine tumors. A prospective phase II study in 24 patients. Cancer 1993;71(8):2624–2630.
Kim YH, Ajani JA, Carrasco CH, Dumas P, Richli W, Lawrence D, Chuang V, Wallace S. Selective hepatic arterial chemoembolization for liver metastases in patients with carcinoid tumor or islet cell carcinoma. Cancer Invest 1999;17(7):474–478.
Perry LJ, Stuart K, Stokes KR, Clouse ME. Hepatic arterial chemoembolization for metastatic neuroendocrine tumors. Surgery 1994;116(6):1111–1116; discussion 1116–1117.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bloomston, M., Al-Saif, O., Klemanski, D. et al. Hepatic Artery Chemoembolization in 122 Patients with Metastatic Carcinoid Tumor: Lessons Learned. J Gastrointest Surg 11, 264–271 (2007). https://doi.org/10.1007/s11605-007-0089-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-007-0089-z