
Abstract
Background
There is no robust evidence of the best operative treatment for displaced unstable metacarpal neck fractures. Numerous constructs are used in the fixation of metacarpal neck fractures. Currently, two common methods are dorsal locking plate and K-wire fixation. A new metacarpal sled fixation system for metacarpal neck fracture was designed to provide fracture stability but limit dissection and avoid exposed hardware. The purpose of this study was to compare the biomechanical integrity of the metacarpal sled versus standard locking plate fixation and retrograde K-wire fixation in a simulated porcine metacarpal fracture model.
Methods
Transverse metacarpal neck fractures were created in 30 porcine second metacarpals. The specimens were randomly fixed with locking plates, metacarpal sleds, or retrograde K-wires. Constructs were then loaded to failure in three-point bending. Stiffness and peak load were measured from the load-to-failure deflection curve. Data were analyzed via ANOVA, followed by Tukey–Kramer’s post hoc pairwise comparison.
Results
The K-wire group had the highest initial stiffness followed by the sled group and then the plate group. Statistical difference was only found between K-wires and plate. Peak load for the K-wire group was lowest, followed by sled, and then by plate. A statistically significant difference was observed between the peak loads of the K-wires and plate, as well as the sled and plate. However, a difference in peak load was not detected between the K-wires and sled.
Conclusions
For transverse metacarpal neck fractures, a metacarpal sled construct provides similar fixation to K-wires with limited dissection and without exposed hardware or the potential for soft tissue tethering. The new low profile construct using a minimally invasive technique would be suitable for unstable metacarpal neck fractures.
Similar content being viewed by others



Introduction
Metacarpal neck fracture, especially of the small finger, is one of the most common injuries of the hand, accounting for 10–30 % of all hand fractures and 25–50 % of all metacarpal bone fractures [2, 13, 20]. Among punching-related ring and little finger metacarpal injuries, over 45 % were to the little finger metacarpal neck [22]. These volarly angulated fractures occur when a clenched metacarpophalangeal joint hits a solid object [25]. While many of these fractures can be managed nonoperatively, unacceptable palmar angulation, open fractures with associated soft tissue injury, and rotational deformity are indications for surgical intervention. The acceptable angulations of the metacarpal neck fractures differ depending on the digits. For the small finger, biomechanical studies have shown that fracture angles more than 30° showed decreased grip strength and efficiency of flexor digiti minimi [1, 3]. In clinical setting, considerable angulation of a small finger metacarpal neck fracture is acceptable without compromising hand function. Angulation of up to 70° can be well tolerated, although in certain patient populations who use their hands extensively for gripping, operative intervention is recommended when the flexion deformity is greater than 40° [25].
The best operative treatment for displaced unstable metacarpal neck fractures is not clearly evident. Fixation methods described in the literature include retrograde K-wire pinning, intermetacarpal transverse K-wires, crossed K-wires, antegrade intramedullary nailing, and fixed angle or locked plating. Each construct has its own advantages and disadvantages. K-wire fixation is fast, respects the soft tissue envelope around the fracture, and is relatively easy. Drawbacks include wire migration, pin tract infection, and tethering of the sagittal bands of the extensor mechanism [5, 8, 24]. Locking plates provide rigid fixation, allowing early range of motion, but limitations include joint and tendon adherence, stiffness, and fibrosis due to the more extensile approach [11]. Multiple studies have shown decreased mean relative range of motion of metacarpophalangeal flexion compared to K-wires [8, 10, 28]. Prominent hardware is also another complication, which can necessitate hardware removal or even result in extensor tendon rupture [18, 24].
Noting the advantages of K-wire fixation but desiring the lower profile construct of internal fixation, a fixation device for distal metacarpal fractures was designed to allow rapid implantation with minimal interference to overlying tendons and soft tissues. This new “sled system” is analogous to a tension band technique that is inserted using two 1-cm incisions so soft tissue dissection is limited. Additionally, the system is completely contained under the extensor mechanism, thus avoiding soft tissue tethering and the risk of pin track infections associated with percutaneous pinning. The goal of this study was to evaluate the biomechanical integrity of the metacarpal sled fixation by comparing it to retrograde intramedullary K-wire fixation and locked plating techniques in a simulated porcine metacarpal fracture model. All constructs were evaluated in bending to failure.
Material and Methods
Thirty fresh frozen second porcine metacarpals, ranging from 62 to 67 mm in length, were used due to their similarity to human metacarpals and to their relative homogeneity as described in previous studies [7, 16, 17]. Specimens were stored at −20 °C and gently warmed to room temperature on the day of the testing. Approximately 12–16 mm of proximal segment of specimens were secured in a 2-in. diameter PVC tube filled with polymethyl methacrylate (PMMA). Under fluoroscopic guidance, the physis of each metacarpalwas identified and osteotomized using a 0.4-mm saw blade to simulate a neck fracture. This fracture distance ranged from 13 to 17 mm from distal articular surface.
Specimens were randomly assigned to three different fixation techniques performed by a single surgeon:
-
Group 1
Ten specimens were stabilized with two 1.1-mm (0.045 in.) diameter K-wires in intramedullary retrograde fashion while using manual axial compression (1.1-mm diameter × 120-mm length, Medical Components Specialists, Bellingham, MA). The K-wires were inserted at the articular cartilage and metacarpal head junction to approximately 38 mm inside the metacarpal from the insertion sites to approximate the same length as the sleds. Wire ends were shortened after fixation to leave 15 mm of length protruding (Fig. 1a).
Fig. 1 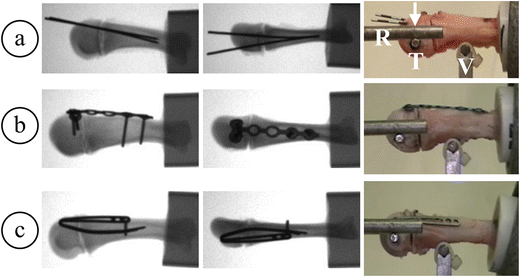
Lateral fluoroscopic images of fixation methods for porcine metacarpal neck fractures repaired via a K-wires, b locking plate, and c sled (left); AP fluoroscopic images (center); specimens mounted on testing apparatus (right). T transverse pin, R loading rod, V vertical support, arrow direction of loading
-
Group 2
Ten specimens were fixed using the T plate system with 2-mm diameter locking screws (TriMed, Santa Clarita, CA). The six-hole plates were cut to 38 mm in length to approximate the length of the sleds. The T plates were placed at the dorsum of the metacarpal with two bicortical proximal locking and two unicortical distal locking screws while using manual compression at the fracture site. The holes were predrilled with 1.7-mm drill (Fig. 1b).
-
Group 3
Ten specimens were fixed with the metacarpal sleds (TriMed, Santa Clarita, CA). The sled intramedullary prongs measure 35 and 38 mm in length, and the extramedullary portion measures 4 mm in width. A 2.0-mm drill was used to create a guide hole at the similar location as the K-wire insertion site on the ulnar dorsal side of the metacarpal head. The sled prongs were then placed into the guide hole and tamped down the intramedullary canal of the metacarpal to compress the fracture. A 1.7-mm bicortical proximal screw was placed in the most proximal hole of the implant (Fig. 1c).

The other proximal screw hole was not used as its’ design intent is as a backup location in the event that sufficient screw purchase is not achieved at the most proximal location.
Specimens were then mounted on a model 1321 biaxial servohydraulic Instron material testing apparatus (Instron Corp., Canton, MA), retrofitted with MTS TestStarII digital controller (MTS Corp., Eden Prairie, MN). Using a custom drill fixture, a 3.2-mm diameter transverse pin was placed horizontally through the distal fragment at approximately 8 mm distal to the fracture and 5 mm volar to the center of the shaft (predrilled with 2.9-mm drill). A volar support was centered under each individual specimen (15 mm proximal from the fracture site) to simulate three-point bending. Two fixed 6.4-mm diameter rods (35 mm apart with one on each side and centered with distal fragment) were lowered to touch the 3.2-mm transverse pin (Fig. 1). The constructs were loaded to failure by displacement at 100 mm/min of the two 6.4-mm rods touching the transverse pin. A load-deflection curve was generated, and initial stiffness was calculated using the slope of the linear region between 20 and 60 N of load. The peak load was identified to compare the ultimate strength of the constructs. Data from specimens were analyzed via an ANOVA with statistical significance set at a p value of ≤0.05, followed by Tukey–Kramer’s post hoc pairwise comparisons (SAS Institute Inc., Cary, NC).
Results
For K-wire constructs, failures were characterized by sliding of the distal fragment down the K-wires. (Fig. 2a). In three constructs, one of the two K-wires cut out of the distal fragment. K-wires remained fixed within the shaft during all trials. For locking plates, nine constructs failed through the distal fragment at the distal locking screws (Fig. 2b). Some bending of the plate at the fracture site was observed in all of these constructs at failure. One construct failed by the distal plate bending and sliding down the side of the shaft. No loosening of the plate/screw interface was observed on the shaft of any of the constructs. Fracture of the shaft at the most proximal screw propagating down toward the volar support was observed in two of the specimens. This differed from the sled in which the sled rotated down the shaft around the proximal screw in nine out of ten constructs. Seven of ten sleds also cut out of the distal fragment. In six specimens, the intramedullary prongs of the sleds were bent at the fracture site. There was no loosening of the proximal screw for any of the sled constructs (Fig. 2c).

Failure mechanisms of the three fixation techniques: a K-wires, b locking plate, and c sled
The K-wires group had the highest initial stiffness (92.51 ± 31.0 N/mm), followed by the sled group (78.46 ± 14.9 N/mm) and then the plate group (61.1 ± 13.7 N/mm). A statistically significant difference was only found between K-wires and plates (p = 0.0076). No statistical significance was observed between K-wires and sleds (p = 0.32) or between sleds and plates (p = 0.18) (Fig. 3).

Stiffness from 20 to 60 N of load of the three fixation methods for the metacarpal neck fracture model
The retrograde K-wires peak load of 154.7 ± 31.2 N was lowest, followed by the sleds group at 205.8 ± 45.3 N, and then by the highest occurring with the plate group at 338.4 ± 71.7 N (Fig. 4). A statistically significant difference was observed between K-wire and plate (p < 0.0001), as well as plate and sled (p < 0.0001). However, a significant difference was not detected between K-wire and sled (p = 0.0908) (Fig. 4).

Peak load of the three fixation methods for the metacarpal neck fracture model
Discussion
This study sought to compare two common fixation methods for metacarpal neck fractures—retrograde intramedullary K-wire fixation and locking plate fixation—to a new sled system. K-wire fixation was found to be the most rigid construct followed by the sled then the locking plate while the locking plate provided the ultimate peak strength. The sled system is analogous to a tension band technique in that it incorporates two prongs inserted into the metacarpal that are connected in an inverted U-fashion on top of the periosteum of the metacarpal and secured with a screw for fixation proximally. The tension band construct has been used successfully in many types of fracture fixation including olecranon fracture, patella fracture, and medial malleolus fracture [6, 19, 23]. In this case, the metacarpal sled simulates a tension band construct where the outer portion of the plate is located on the tension side of the fracture so that normal flexion forces across the metacarpal compresses the fracture. Similar sled constructs have been commercially available for fixation of medial malleolus ankle fracture and olecranon fracture [6, 15].
No biomechanical study has previously compared peak load and stiffness of K-wires to locking plate fixation in a metacarpal neck fracture model. Firoozbakhsh and colleagues compared various fixation techniques for metacarpal fractures including dorsal plating, crossed K-wires with tension banding, and intramedullary paired 0.045-in. K-wires [9]. These constructs were tested with cyclic four-point bending in an oblique metacarpal shaft fracture model. The dorsal plate with lag screw was reported as superior in all modes of testing. Plate fatigue life and peak load in bending was superior, followed by crossed K-wire tension banding and intramedullary K-wire fixation. Initial rigidity for the plate was superior to the K-wire constructs though there was no difference between intramedullary K-wires and the tension band construct. Another study compared the fixation of simulated transverse metacarpal fractures between dorsal plating with and without lag screws and various K-wire fixations in three-point bending. The plate constructs demonstrated significantly higher dorsal bending rigidity and peak loads while the various K-wire constructs all had similar biomechanical characteristics [4]. The findings of our study are consistent with prior literature in regard to peak load but differed in that the initial stiffness of our plated constructs were significantly lower than K-wires. The lower initial stiffness for the plate is likely due to the location of the transverse fracture at the physis, the use of locking screws, and the lack of an interfragmentary lag screw with the plate. As a result, some initial bone movement occurred before the plate firmly engaged but once fully engaged, allowed for a higher peak load before failing.
Compared to dorsal locking plate, lower peak loads of the sled is not surprising when taking into account the increased amount of hardware involved with plates. There is no literature to suggest that this level of fracture stability is necessary for healing and, in fact, the dissection necessary to implant this type of fixation may add significant morbidity. Facca and colleagues showed decreased mean relative range of motion of metacarpophalangeal flexion in plating, increased stiffness/fibrosis, and rare metacarpal head necrosis [8]. Limiting soft tissue trauma should offer improved rehabilitation potential following metacarpal fixation as long as adequate stability is achieved. Prominent hardware is another drawback of the locking plate fixation and possibly causes extensor tendon damage [18]. Although the sled may appear prominent in the porcine metacarpal model, this has more to do with the shape of porcine metacarpals and the sled has a much lower profile on human metacarpals.
The sled construct, on the other hand, did provide equivalent fracture fixation for simulated metacarpal neck fractures as K-wires. Clinically, K-wire fixation is adequate to maintain fracture reduction during healing but has many disadvantages related primarily to its percutaneous nature. Botte et al. showed that 5 % of patients sustained major complications, 11 % sustained minor complications, and an additional 2 % of patients had both minor and major complications associated with K-wire fixation [5]. Hargreaves demonstrated that exposed K-wires have a higher infection risk than buried hardware [12]. Though K-wires can be cut and buried underneath the skin, Hsu et al. detected no difference in the incidence of infection between K-wires that were left exposed or buried beneath skin. Buried K-wires can be irritating to overlying soft tissue, can impinge on the extensor mechanism, and can puncture the skin and become exposed even when initially buried. In Hsu’s review of 408 smooth pins, there was total of 14 % complication rate, mostly infection but includes pin loosening, migration, delayed wound healing, and drainage [14]. Other studies have also noted 17 % pin site infection risk and 3–4 % K-wire migration rates [14, 26].
The ultimate question is, of course, how much stability is necessary to ensure adequate healing of metacarpal fractures. Once this level of stability is determined, then strategies can be designed to achieve this goal as efficiently and with as little morbidity as possible. Most likely this “sweet spot” of stability is variable and depends on fracture patterns, soft tissue stripping, individual physiological differences, as well as the stresses placed on the healing fracture by protected and unprotected patient activities. We chose to compare the metacarpal sled to K-wire fixation and locking plate fixation based on the perception that K-wire fixation offered the least stability necessary to allow healing while locking plate fixation (also clinically effective) provided the opposite extreme of fixation strength. A recent meta-analysis comparing these two forms of fixation in 1375 patients noted the superiority of plate fixation but cited infection and stiffness (related to postoperative immobilization) as two main problems (rather than nonunion) with K-wire fixation [27]. Our biomechanical findings suggest that if K-wire fixation stability is sufficient to allow fracture healing, then the metacarpal sled should provide adequate stability while avoiding many of the problems associated with K-wire fixation.
There are limitations to this study. Similar to other in vitro biomechanical studies, surrounding soft tissue and in vivo healing behavior was not simulated. The three-point bending loads applied to the metacarpal neck were meant to mimic the most common deforming forces—flexion forces from intrinsic and extrinsic flexors as has been simulated in prior metacarpal fracture studies [7, 16, 17]. However, due to the location of the fracture and associated hardware, the metacarpal head could not be loaded directly dorsally. We selected to use transverse pin fixation to the metacarpal head and load the transverse pin instead. Transverse pin deflection was accounted for in our data analysis. A fulcrum or waist was also necessary to focus the applied forces to the hardware–bone interface (as opposed to the PMMA–bone interface). Additionally, this model did not access rotational stability though future studies could further characterize the biomechanical behavior in other modes of loading. Porcine metacarpals were used to approximate a human model and have been used in other metacarpal fracture studies [7, 16, 17]. Human cadaver specimens have drawbacks due to their diverse variation in bone density and quality. Sawbones are homogenous but may have the disadvantage of lacking some of the biologic variety that is found clinically. Fracture reduction was challenging with locking plates because the locking screws do not pull the plate to the bone in the manner of conventional screws [21]. The plate was not perfectly contoured to the metacarpal head. The unicortical locking screws in the metacarpal head were short, and longer screws may have increased the load to failure.
Based on this study, the sled construct is a fixation method for metacarpal neck fractures that provided at least a similar strength and rigidity profile to K-wire fixation. The sled offers limited dissection without exposed hardware or soft tissue tethering. Additional in vivo studies will be necessary to make definitive conclusions regarding clinical effectiveness.
References
Ali A, Hammam J, Mass DP. The biomechanical effects of angulated boxer’s fractures. J Hand Surg [Am]. 1999;24:835–44. doi:10.1053/jhsu.1999.0835.
Anakwe RE, Aitken SA, Cowie JG, et al. The epidemiology of fractures of the hand and the influence of social deprivation. J Hand Surg Eur. 2011;36:62–5. doi:10.1177/1753193410381823.
Birndorf MS, Daley R, Greenwald DP. Metacarpal fracture angulation decreases flexor mechanical efficiency in human hands. Plast Reconstr Surg. 1997;99:1079–83. doi:10.1097/00006534-199704000-00024. discussion 1084-5.
Black D, Mann RJ, Constine R, et al. Comparison of internal fixation techniques in metacarpal fractures. J Hand Surg [Am]. 1985;10:466–72. doi:10.1016/S0363-5023(85)80067-8.
Botte MJ, Davis JL, Rose BA, et al. Complications of smooth pin fixation of fractures and dislocations in the hand and wrist. Clin Orthop Relat Res. 1992;276:194–201. doi:10.1097/00003086-199203000-00025.
Della Rocca GJ. Displaced patella fractures. J Knee Surg. 2013;26:293–9. doi:10.1055/s-0033-1353988.
Doht S, Jansen H, Meffert RH, et al. Higher stability with locking plates in hand surgery? Biomechanical investigation of the TriLock system in a fracture model. Int Orthod. 2012;36:1641–6. doi:10.1007/s00264-012-1524-7.
Facca S, Ramdhian R, Pelissier A, et al. Fifth metacarpal neck fracture fixation: locking plate versus K-wires? Orthop Traumatol Surg Res. 2010;96:506–12. doi:10.1016/j.otsr.2010.02.009.
Firoozbakhsh KK, Moneim MS, Howey T, et al. Comparative fatigue strengths and stabilities of metacarpal internal fixation techniques. J Hand Surg [Am]. 1993;18:1059–68. doi:10.1016/0363-5023(93)90403-P.
Fujitani R, Omokawa S, Shigematsu K, et al. Comparison of the intramedullary nail and low-profile plate for unstable metacarpal neck fractures. J Orthop Sci. 2012;17:450–6. doi:10.1007/s00776-012-0223-y.
Fusetti C, Meyer H, Borisch N, et al. Complications of plate fixation in metacarpal fractures. J Trauma. 2002;52:535–9. doi:10.1097/00005373-200203000-00019.
Hargreaves DG, Drew SJ, Eckersley R. Kirschnerwire pin tract infection rates: a randomized controlled trial between percutaneous and buried wires. J Hand Surg (Br). 2004;29:374–6. doi:10.1016/j.jhsb.2004.03.003.
Hove LM. Fractures of the hand. Distribution and relative incidence. Scand J Plast Reconstr Surg Hand Surg. 1993;27:317–9.
Hsu LP, Schwart EG, Kalainov DM, et al. Complications of K-wire fixation in procedures involving the hand and wrist. J Hand Surg [Am]. 2011;36:610–6. doi:10.1016/j.jhsa.2011.01.023.
Iorio T, Wong JC, Patterson JD, et al. Olecranon osteotomy fixation using a novel device: the olecranon sled. Tech Hand Up Extrem Surg. 2013;17:151–7. doi:10.1097/BTH.0b013e318298b39d.
Mudrick CA, Owen JR, Wayne JS, et al. Unicortical PEEK inset locking fixation for metacarpal fractures: a biomechanical study. Eur J Orthop Surg Traumatol. 2013. doi:10.1007/s00590-013-1322-y.
Ochman S, Doht S, Paletta J, et al. Comparison between locking and non-locking plates for fixation of metacarpal fractures in an animal model. J Hand Surg [Am]. 2010;35:597–603. doi:10.1016/j.jhsa.2010.01.002.
Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg [Am]. 1998;23:827–32. doi:10.1016/S0363-5023(98)80157-3.
Patel T, Owen JR, Byrd WA, et al. Biomechanical performance of a new device for medial malleolar fractures. Foot Ankle Int. 2013;34:426–33. doi:10.1177/1071100712466231.
Schädel-Höpfner M, Wild M, Windolf J, et al. Antegrade intramedullary splinting or percutaneous retrograde crossed pinning for displaced neck fractures of the fifth metacarpal? Arch Orthop Trauma Surg. 2007;127:435–40. doi:10.1007/s00402-006-0254-y.
Smith WR, Ziran BH, Anglen JO, et al. Locking plates: tips and tricks. J Bone Joint Surg Am. 2007;89:2298–307. Review.
Soong M, Got C, Katarincic J. Ring and little finger metacarpal fractures: mechanisms, locations, and radiographic parameters. J Hand Surg [Am]. 2010;35:1256–9. doi:10.1016/j.jhsa.2010.05.013.
Veillette CJ, Steinmann SP. Olecranon fractures. Orthop Clin North Am. 2008;39:229–36. doi:10.1016/j.ocl.2008.01.002.
Weinstein LP, Hanel DP. Metacarpal fractures. J Am Soc Surg Hand. 2002;2:168–80. doi:10.1053/jssh.2002.36788.
Wolfe SW, Hotchkiss RN, Pederson WC, et al. Metacarpal neck fracture. Green’s Oper Hand Surg. 6th edition, 2011; 241.
Wong TC, Ip FK, Yeung SH. Comparison between percutaneous transverse fixation and intramedullary K-Wires in treating closed fractures of the metacarpal neck of the little finger. J Hand Surg (Br). 2006;31:61–5. doi:10.1016/j.jhsb.2005.06.022.
Xu J, Zhang C. Mini-plate versus Kirschner wire internal fixation for treatment of metacarpal and phalangeal fractures in Chinese Han population: a meta-analysis. J Orthop Surg Res. 2014;9:24. doi:10.1186/1749-799X-9-24.
Zemirline A, Vaiss L, Lebailly F, et al. The MetaHUS(®) fixation system versus pinning and plating in 5th metacarpal neck fractures. Chir Main. 2014;33:207–10. doi:10.1016/j.main.2014.04.003.
Acknowledgments
Blinded for the review.
Conflict of Interest
Pramote Malasitt, John R. Owen, Marc-Antoine Tremblay, Jennifer S. Wayne, and Jonathan E. Isaacs certify that they have no commercial associations (e.g., consultancies, stock ownership, equity interest, and patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article. Jonathan E. Isaacs is a consultant for TriMed, Inc. Hardware required for this study was provided by TriMed, Inc., Santa Clarita, CA. Partial financial support was received from Medarva Healthcare Richmond, VA.
Statement of Human and Animal Rights
No living subjects were used in this study. Institutional procedures were followed in the handling of cadaveric specimens.
Statement of Informed Consent
Not applicable.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Malasitt, P., Owen, J.R., Tremblay, MA. et al. Fixation for metacarpal neck fracture: a biomechanical study. HAND 10, 438–443 (2015). https://doi.org/10.1007/s11552-015-9744-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11552-015-9744-0