
Abstract
Aim
To assess the amount of computed tomography (CT) scans for minor head injury (MHI) performed in young patients in our emergency department (ED), not indicated by National Institute for Health and Clinical Excellence (NICE) and Canadian Computed Tomography Head Rules (CCHR), and to analyze factors contributing to unnecessary examinations. Secondary objectives were to calculate the effective dose, to establish the number of positive CT and to analyze which of the risk factors are correlated with positivity at CT; finally, to calculate sensitivity and specificity of NICE and CCHR in our population.
Materials and methods
We retrospectively evaluated 493 CT scans of patients aged 18–45 years, collecting the following parameters from ED medical records: patient demographics, risk factors indicating the need of brain imaging, trauma mechanism, specialty and seniority of the referring physician. For each CT, the effective dose and the negativity/positivity were assessed.
Results
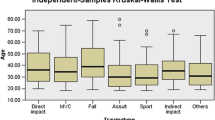
357/493 (72%) and 347/493 (70%) examinations were not in line with the CCHR and NICE guidelines, respectively. No statistically significant difference between physician specialty (p = 0.29 for CCHR; p = 0.24 for NICE), nor between physician seniority and the amount of inappropriate examinations (p = 0.93 for CCHR, p = 0.97 for NICE) was found but CT scans requested by ED physicians were less inappropriate [p = 0.28, odds ratio (OR) 0.562, CI (95%) 0.336–0.939]. There was no statistically significant correlation between patient age and over-referral (p = 0.74 for NICE, p = 0.93 for CCHR). According to NICE, low speed motor vehicle accident (p = 0.009), motor vehicle accident with high energy impact (p < 0.01) and domestic injuries (p = 0.002) were associated with a higher rate of unwarranted CT; according to CCHR only motor vehicle accident with high energy impact showed a significant correlation with unwarranted CT scan (p < 0.001, OR 44.650, CI 33.123–1469.854). 2% of CT was positive. Multivariate analysis demonstrated that factors significantly associated with CT scan positivity included signs of suspected skull fracture (p < 0.001, OR 20.430, CI 2.727–153.052) and motor vehicle accident with high energy impact (p < 0.001, OR 220.650, CI 33.123–1469.854). In our series, CCHR showed sensitivity of 100%, specificity of 74%; NICE showed sensitivity of 100%, specificity of 72%.
Conclusion
We observed an important overuse of head CT scans in MHI; the main promoting factor for inappropriate was injury mechanism. 2% of head CT were positive, correlating with signs of suspected skull fracture and motor vehicle accident with high energy impact.
Similar content being viewed by others


References
Morton MJ, Korley FK (2012) Head computed tomography use in the emergency department for mild traumatic brain injury: integrating evidence into practice for the resident physician. Ann Emerg Med 60(3):361–367
Smits M, Dippel DW, Nederkoorn PJ, Dekker HM, Vos PE, Kool DR, van Rijssel DA, Hofman PA, Twijnstra A, Tanghe HL, Hunink MG (2010) Minor head injury: CT-based strategies for management—a cost-effectiveness analysis. Radiology 254(2):532–540
Stiell IG, Wells GA, Vandemheen K, Clement C, Lesiuk H, Laupacis A, McKnight RD, Verbeek R, Brison R, Cass D, Eisenhauer ME, Greenberg G, Worthington J (2001) The Canadian CT Head Rule for patients with minor head injury. Lancet 357(9266):1391–1396
Papa L, Stiell IG, Clement CM, Pawlowicz A, Wolfram A, Braga C, Draviam S, Wells GA (2012) Performance of the Canadian CT Head Rule and the New Orleans Criteria for predicting any traumatic intracranial injury on computed tomography in a United States Level I trauma center. Acad Emerg Med 19(1):2–10
Haydon NB (2013) Head injury: audit of a clinical guideline to justify head CT. J Med Imaging Radiat Oncol 57(2):161–168
Griffey RT, Sodickson A (2009) Cumulative radiation exposure and cancer risk estimates in emergency department patients undergoing repeat or multiple CT. AJR Am J Roentgenol 192(4):887–892
Haydel MJ, Preston CA, Mills TJ, Luber S, Blaudeau E, DeBlieux PM (2000) Indications for computed tomography in patients with minor head injury. N Engl J Med 343(2):100–105
Sadegh R, Karimialavijeh E, Shirani F, Payandemehr P, Bahramimotlagh H, Ramezani M (2016) Head CT scan in Iranian minor head injury patients: evaluating current decision rules. Emerg Radiol 23(1):9–16
National Clinical Guideline Centre (UK) (2014) Head injury: triage, assessment, investigation and early management of head injury in children, young people and adults. National Institute for Health and Clinical Excellence: Guidance
Jagoda AS, Bazarian JJ, Bruns JJ Jr, Cantrill SV, Gean AD, Howard PK, Ghajar J, Riggio S, Wright DW, Wears RL, Bakshy A, Burgess P, Wald MM, Whitson RR (2008) American College of Emergency Physicians; Centers for Disease Control and Prevention Clinical policy: neuroimaging and decision making in adult mild traumatic brain injury in the acute setting. Ann Emerg Med 52(6):714–748
Servadei F, Teasdale G, Merry G (2001) Neurotraumatology Committee of the World Federation of Neurosurgical Societies. Defining acute mild head injury in adults: a proposal based on prognostic factors, diagnosis, and management. J Neurotrauma 18(7):657–664
Mower WR, Hoffman JR, Herbert M, Wolfson AB, Pollack CV Jr, Zucker MI, NEXUS II Investigators (2002) National Emergency X-Radiography Utilization Study. Developing a clinical decision instrument to rule out intracranial injuries in patients with minor head trauma: methodology of the NEXUS II investigation. Ann Emerg Med 40(5):505–514
Harnan SE, Pickering A, Pandor A, Goodacre SW (2011) Clinical decision rules for adults with minor head injury: a systematic review. J Trauma 71(1):245–251
Sodickson A, Baeyens PF, Andriole KP, Prevedello LM, Nawfel RD, Hanson R, Khorasani R (2009) Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 251(1):175–184
Fabbri A, Servadei F, Marchesini G, Dente M, Iervese T, Spada M, Vandelli A (2005) Clinical performance of NICE recommendations versus NCWFNS proposal in patients with mild head injury. J Neurotrauma 22(12):1419–1427
Melnick ER, Shafer K, Rodulfo N, Shi J, Hess EP, Wears RL, Qureshi RA, Post LA (2015) Understanding overuse of computed tomography for minor head injury in the emergency department: a triangulated qualitative study. Acad Emerg Med 22(12):1474–1483
Schueller G, Scaglione M, Linsenmaier U, Schueller-Weidekamm C, Andreoli C, De Vargas MM, Gualdi G (2015) The key role of the radiologist in the management of polytrauma patients: indications for MDCT imaging in emergency radiology. Radiol Med 120(7):641–654
Jame SZB, Majdzadeh R, Sari AA, Rashidian A, Arab M, Rahmani H (2014) Indications and overuse of computed tomography in minor head trauma. Iran Red Crescent Med J 16(5):e13067
Klang E, Beytelman A, Greenberg D, Or J, Guranda L, Konen E, Zimlichman E (2017) Overuse of Head CT examinations for the investigation of minor head trauma: analysis of contributing factors. J Am Coll Radiol 14(2):171–176
Melnick ER, Szlezak CM, Bentley SK, Dziura JD, Kotlyar S, Post LA (2012) CT overuse for mild traumatic brain injury. Jt Comm J Qual Patient Saf 38(11):483–489
Natale JE, Joseph JG, Rogers AJ, Mahajan P, Cooper A, Wisner DH, Miskin ML, Hoyle JD Jr, Atabaki SM, Dayan PS, Holmes JF, Kuppermann N, PECARN (Pediatric Emergency Care Applied Research Network) (2012) Cranial computed tomography use among children with minor blunt head trauma: association with race/ethnicity. Arch Pediatr Adolesc Med 166(8):732–737
Fortin EM, Fisher J, Qiu S, Babcock CI (2016) Privately insured medical patients are more likely to have a head CT. Emerg Radiol 23(6):597–601
Lee J, Evans CS, Singh N, Kirschner J, Runde D, Newman D, Wiener D, Quaas J, Shah K (2013) Head computed tomography utilization and intracranial hemorrhage rates. Emerg Radiol 20(3):219–223
Borczuk P (1995) Predictors of intracranial injury in patients with mild head trauma. Ann Emerg Med 25(6):731–736
Gómez PA, Lobato RD, Ortega JM, De La Cruz J (1996) Mild head injury: differences in prognosis among patients with a Glasgow Coma Scale score of 13–15 and analysis of factors associated with abnormal CT findings. Br J Neurosurg 10(5):453–460
Bouida W, Marghli S, Souissi S, Ksibi H, Methammem M, Haguiga H, Khedher S, Boubaker H, Beltaief K, Grissa MH, Trimech MN, Kerkeni W, Chebili N, Halila I, Rejeb I, Boukef R, Rekik N, Bouhaja B, Letaief M, Nouira S (2013) Prediction value of the Canadian CT Head Rule and the New Orleans criteria for positive head CT scan and acute neurosurgical procedures in minor head trauma: a multicenter external validation study. Ann Emerg Med 61(5):521–527
Wu SR, Shakibai S, McGahan JP, Richards JR (2006) Combined head and abdominal computed tomography for blunt trauma: which patients with minor head trauma benefit most? Emerg Radiol 13(2):61–67
Khaji A, Eftekhar B, Karbakhsh M, Ardalan KM (2006) The use of head CT scanning in mild head injury. Neurosciences (Riyadh) 11(4):248–251
af Geijerstam JL, Britton M (2003) Mild head injury—mortality and complication rate: meta-analysis of findings in a systematic literature review. Neurochirurgica (Wien) 145(10):843–850 (discussion 850)
Brenner DJ, Elliston CD (2004) Estimated radiation risks potentially associated with full-body CT screening. Radiology 232(3):735–738
Salerno S, Marrale M, Geraci C, Caruso G, Re GL, Casto AL, Midiri M (2016) Cumulative doses analysis in young trauma patients: a single-centre experience. Radiol Med 121(2):144–152
Giannitto C, Campoleoni M, Maccagnoni S, Angileri AS, Grimaldi MC, Giannitto N, De Piano F, Ancona E, Biondetti PR, Esposito AA (2018) Unindicated multiphase CT scans in non-traumatic abdominal emergencies for women of reproductive age: a significant source of unnecessary exposure. Radiol Med 123(3):185–190
Vrijheid M, Cardis E, Ashmore P, Auvinen A, Bae JM, Engels H, Gilbert E, Gulis G, Habib R, Howe G, Kurtinaitis J, Malker H, Muirhead C, Richardson D, Rodriguez-Artalejo F, Rogel A, Schubauer-Berigan M, Tardy H, Telle-Lamberton M, Usel M, Veress K (2007) Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers. Int J Epidemiol 36(5):1126–1135
Cardis E, Vrijheid M, Blettner M, Gilbert E, Hakama M, Hill C, Howe G, Kaldor J, Muirhead CR, Schubauer-Berigan M, Yoshimura T, Bermann F, Cowper G, Fix J, Hacker C, Heinmiller B, Marshall M, Thierry-Chef I, Utterback D, Ahn YO, Amoros E, Ashmore P, Auvinen A, Bae JM, Solano JB, Biau A, Combalot E, Deboodt P, Diez Sacristan A, Eklof M, Engels H, Engholm G, Gulis G, Habib R, Holan K, Hyvonen H, Kerekes A, Kurtinaitis J, Malker H, Martuzzi M, Mastauskas A, Monnet A, Moser M, Pearce MS, Richardson DB, Rodriguez-Artalejo F, Rogel A, Tardy H, Telle-Lamberton M, Turai I, Usel M, Veress K (2005) Risk of cancer after low doses of ionising radiation: retrospective cohort study in 15 countries. BMJ 331(7508):77
Funding
No funding has been received for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no conflict of interest.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Institutional review board approval was granted for this retrospective study with a waiver of the requirement to obtain written informed consent from each patient.
Rights and permissions
About this article

Cite this article
Cellina, M., Panzeri, M., Floridi, C. et al. Overuse of computed tomography for minor head injury in young patients: an analysis of promoting factors. Radiol med 123, 507–514 (2018). https://doi.org/10.1007/s11547-018-0871-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-018-0871-x