
Abstract
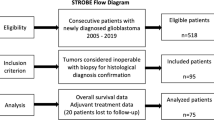
The extent of surgery predicts overall survival (OS) in patients treated for glioblastoma (GBM). The therapeutic approach after partial resection (PR) or biopsy alone (BA) is not clearly defined. This retrospective analysis was therefore planned to analyse clinical features, treatment and survival of patients undergoing PR or BA. We analysed the clinical/therapeutic features and the outcome of 232 patients submitted to BA/PR and treated with radiotherapy (RT) with/without chemotherapy. Two subgroups (pre- and post-Temozolomide-era) were identified. The BA/PR ratio did not change with the accrual periods. In the TMZ-era, 50 % of the patients had chemotherapy; “small” volume, hypo-fractionated and “low” dose RT (<54 Gy) were delivered to 93, 38 and 44 % of the patients; corresponding values for the previous period were 4, 28, 11 and 2 % (P < 0.001). Better two-year OS was evident in the TMZ-era (18 vs 7 %); PR and chemotherapy affected OS in patients treated with hypo-fractionated, low doses RT (P = 0.02, 0.04). Limited volume, more often MRI-based, and “short” RT treatments were given mostly to unfavourably selected patients, without compromising the results of the whole group. This strategy, combined with an increased use of chemotherapy, resulted in reduced treatment burden, in an improved 2-year OS rate and prospectively in better quality of life, even in this prognostically worse subset of glioma patients.
Similar content being viewed by others
References
Devaux BC, O’Fallon JR, Kelly PJ (1993) Resection, biopsy and survival in malignant glial neoplasms. A retrospective study of clinical parameters, therapy, and outcome. J Neurosurg 78:767–775
Gauden AJ, Hunn A, Erasmus A, Waites P, Dubey A, Gauden SJ (2009) Combinated modality treatment of newly diagnosed glioblastoma multiforme in a regional neurosurgical centre. J Clin Neurosci 16:1174–1179
Vuorinen V, Hinkka S, Färkkilä M, Jääskeläinen J (2003) Debulking or biopsy of malignant glioma in elderly people—a randomised study. Acta Neurochir 145(1):5–10
Helseth R, Helseth E, Johannesen TB, Langberg CW, Lote K, Rønning P, Rønning P, Scheie D, Vik A, Meling TR (2010) Overall survival, prognostic factors, and repeated surgery in a consecutive series of 516 patients with glioblastoma multiforme. Acta Neurol Scand 122:159–167
Magrini SM, Ricardi U, Santoni R, Krengli M, Lupattelli M, Cafaro I, Scoccianti S, Menichelli C, Bertoni F, Enrici RM, Tombolini V, Buglione M, Pirtoli L (2006) Pattern of practice and survival in a retrospective analysis of 1722 adult astocytoma patients treated between 1985 and 2001 in 12 italian radiation oncology centers. Int J Radiat Oncol Biol Phys 65:788–799
Lorenzoni J, Torrico A, Villanueva P, Gederlini A, Torrealba G (2008) Surgery for high-grade gliomas in a developing country: survival estimation using a simple stratification system. Surg Neurol 70:591–597
Hess KR (1999) Extent of resection as a prognostic variable in the treatment of gliomas. J Neurooncol 42:227–231
Kreth FW, Warnke PC, Scheremet R, Ostertag CB (1993) Surgical resection and radiation therapy versus biopsy and radiation therapy in the treatment of glioblastoma multiforme. J Neurosurg 78:762–766
Lacroix M, Abi-Said M, Daryl R, Fourney M, Shi W, DeMonte F, Lang FF, McCutcheon IE, Hassenbusch SJ, Holland E, Hess K, Michael C, Miller D, Sawaya R (2001) A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg 95:190–198
Simpson JR, Horton J, Scott C, Curran WJ, Rubin P, Fischbach J, Isaacson S, Rotman M, Asbell SO, Nelson JS (1993) Influence of location and extent of surgical resection on survival of patients with glioblastoma multiforme: results of three consecutive Radiation Therapy Oncology Group (RTOG) clinical trials. Int J Radiat Oncol Biol Phys 26:239–244
Stark W, Stepper W, Mehdorn HM (2010) Outcome evaluation in glioblastoma patients using different ranking scores: KPS, GOS, mRS and MRC. Eur J Cancer Care 19:39–44
McGirt MJ, Chaichana KL, Gathinji M, Attenello FJ, Than K, Olivi A, Weingart JD, Brem H, Quiñones-Hinojosa AR (2009) Independent association of extent of resection with survival in patients with malignant brain astrocytoma. J Neurosurg 110:156–162
Sanai N, Polley MP, McDermott MW, Parsa AT, Berger MS (2011) An extent of resection threshold for newly diagnosed glioblastomas. J Neurosurg 115:3–8
Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO (2009) Effect of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomized phase III study: 5 year analysis of the EORTC-NCIC trial. Lancet Oncol 10:459–466
Chamberlain MC, Chalmers L (2007) A pilot study of primary temozolomide chemotherapy and deferred radiotherapy in elderly patients with glioblastoma. J Neuroncol 82:207–209
Minniti G, De Sanctis V, Muni R, Rasio D, Lanzetta G, Bozza O, Osti MF, Salvati M, Valeriani M, Cantore GP, Maurizi Enrici R (2009) Hypofractionated radiotherapy followed by adjuvant chemotherapy with temozolomide in elderly patients with glioblastoma. J Neuroncol 91:95–100
Marko NF, Weil RJ, Schroeder JL, Lang FF, Suki D, Sawaya R (2014) Extent of resection of glioblastoma revisited: personalized survival modeling facilitates more accurate survival prediction and supports maximum safe resection approach to surgery. J Clin Oncol 32:774–782
Scoccianti S, Magrini SM, Ricardi U, Detti B, Buglione M, Sotti G, Krengli M, Maluta S, Parisi S, Bertoni F, Mantovani C, Tombolini V, De Renzis C, Lioce M, Fatigante L, Fusco V, Muto P, Berti F, Rubino G, Cipressi S, Fariselli L, Lupatteli M, Santoni R, Pirtoli L, Biti GP (2010) Pattern of care and survival in a retrospective analysis of 1059 patients with glioblastoma multiforme treated between 2002 and 2007: a multicenter study by the Central Nervous System Study Group of Airo (Italian Association of Radiation Oncology). Neurosurgery 67:446–458
Conflict of interest
The authors report no declaration of conflict of interest concerning the materials and methods used in this study or the findings specified in this paper.
Ethical standards
“All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards”.
Informed consent
“For this type of study (retrospective), formal consent is not required”.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Buglione, M., Borghetti, P., Pedretti, S. et al. Post-surgical therapeutic approaches to glioblastoma patients submitted to biopsy (BA) or “partial” resection (PR): the possibilities to treat also them without renunciations. Study from the Brescia Neuro-Oncology Group. Radiol med 120, 975–981 (2015). https://doi.org/10.1007/s11547-015-0528-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-015-0528-y