
Abstract
This study was undertaken to prospectively determine the diagnostic capabilities of magnetic resonance (MR) imaging in detecting myometrial and cervical invasion and lymph node involvement in endometrial carcinoma and to identify the causes of errors in staging endometrial carcinoma.
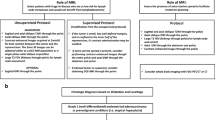
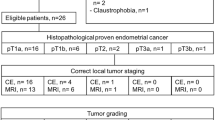
Materials and methods
Twenty consecutive patients with a histological diagnosis of endometrial carcinoma underwent preoperative MR imaging. MR findings were compared with surgical staging, considered as the standard of reference.
Results
In assessing myometrial invasion, MR imaging showed 70% accuracy, 80% sensitivity, 40% specificity, 80% positive predictive value (PPV), and 40% negative predictive value (NPV). In detecting cervical invasion, MR imaging had 95% accuracy, 100% sensitivity, 94.4% specificity, 66.7% PPV, and 100% NPV. In evaluating lymph node involvement, MR imaging showed 100% accuracy, sensitivity, specificity, PPV and NPV. Errors in evaluating myometrial invasion were caused by polypoid tumour, adenomyosis and leiomyomas, whereas those in evaluating cervical invasion were caused by dilatation and curettage.
Conclusions
MR imaging is a reliable technique for preoperative evaluation of endometrial carcinoma. Its main limitation is differentiating between stage IA and IB carcinomas, which is not highly important for surgical planning. Cooperation between the gynaecologist and radiologist is mandatory to avoid staging errors.
Riassunto
Obiettivo
Scopo del presente lavoro è stato determinare prospettivamente le capacità diagnostiche della risonanza magnetica (RM) nel valutare l’invasione del miometrio, della cervice ed il coinvolgimento linfonodale nel carcinoma dell’endometrio ed identificare le cause di errore nella stadiazione RM.
Materiali e metodi
Venti pazienti consecutive con diagnosi istologica di carcinoma dell’endometrio sono state sottoposte ad esame RM preoperatorio. I reperti RM sono stati confrontati con la stadiazione chirurgica considerata come standard di riferimento.
Risultati
Nel valutare l’invasione del miometrio la RM ha mostrato accuratezza del 70%, sensibilità dell’80%, specificità del 40%, valore predittivo positivo (VPP) dell’80%, valore predittivo negativo (VPN) del 40%. Nell’identificare l’infiltrazione della cervice la RM ha mostrato accuratezza del 95%, sensibilità del 100%, specificità del 94,4%, VPP del 66,7%, VPN del 100%. Nel valutare il coinvolgimento linfonodale la RM ha mostrato accuratezza, sensibilità, specificità, VPP e VPN del 100%. Le cause di errore nella valutazione del miometrio sono state: tumore polipoide, adenomiosi, leiomiomi; nella valutazione della cervice: raschiamento.
Conclusioni
La RM è una tecnica affidabile nella valutazione preoperatoria del carcinoma dell’endometrio; il suo limite principale è rappresentato dalla distinzione fra stadio IA e IB, poco influente sulla strategia chirurgica. La collaborazione fra clinico e radiologo è fondamentale per evitare errori di stadiazione.
Similar content being viewed by others
References/Bibliografia
Koyama T, Tamai K, Togashi K (2007) Staging of carcinoma of the uterine cervix and endometrium. Eur Radiol 17:2009–2019
Pakkal MV, Rudralingam V, McCluggage WG, Kelly BE (2004) MR staging in carcinoma of the endometrium and carcinoma of the cervix. Ulster Med J 73:20–24
Sironi S, Taccagni G, Garancini P et al (1992) Myometrial invasion by endometrial carcinoma: assessment by MR imaging. AJR Am J Roentgenol 158:565–569
Kinkel K, Kaji Y, Yu KK et al (1999) Radiologic staging in patients with endometrial cancer: a meta-analysis. Radiology 212:711–718
Piver MS, Rutledge F, Smith JP (1974) Five classes of extended hysterectomy for women with cervical cancer. Obstet Gynecol 44:265–272
Sanjuán A, Escaramís G, Ayuso JR et al (2008) Role of magnetic resonance imaging and cause of pitfalls in detecting myometrial invasion and cervical involvement in endometrial cancer. Arch Gynecol Obstet 278:535–539
Manfredi R, Mirk P, Maresca G et al (2004) Local-regional staging of endometrial carcinoma: role of MR imaging in surgical planning. Radiology 231:372–37
Sobin LH, Gospodarowicz MK, Wittekind Ch (2009) TNM classification of malignant tumours. Wiley-Blackwell, Hoboken, USA
Lin G, Ng KK, Chang CJ et al (2009) Myometrial invasion in endometrial cancer: diagnostic accuracy of diffusion-weighted 3.0-T MR imaging — Initial experience. Radiology 250:784–792
Inada Y, Matsuki M, Nakai G et al (2009) Body diffusion-weighted MR imaging of uterine endometrial cancer: is it helpful in the detection of cancer in nonenhanced MR imaging? Eur J Radiol 70:122–127
Rechichi G, Galimberti S, Signorelli M et al (2010) Myometrial invasion in endometrial cancer: diagnostic performance of diffusion-weighted MR imaging at 1.5-T. Eur Radiol 20:754–762
Harisinghani MG, Saini S, Slater GJ et al (1997) MR imaging of pelvic lymph nodes in primary pelvic carcinoma with ultrasmall superparamagnetic iron oxide (Combidex): preliminary observations. J Magn Reson Imaging 7:161–163
Harisinghani MG, Barentsz J, Hahn PF et al (2003) Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med 348:2491–2499
Rockall AG, Sohaib SA, Harisinghani MG et al (2005) Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J Clin Oncol 23:2813–2821
Hamm B, Kubik-Huch RA, Fleige B (1999) MR imaging and CT of the female pelvis: radiologic-pathologic correlation. Eur Radiol 9:3–15
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Foti, P.V., Farina, R., Coronella, M. et al. Endometrial carcinoma: MR staging and causes of error. Radiol med 118, 487–503 (2013). https://doi.org/10.1007/s11547-012-0861-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-012-0861-3