
Abstract
Purpose
The aim of study was to evaluate the results of our experience with transarterial embolization based on a modified algorithm in patients with splenic injury.
Materials and methods
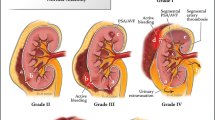
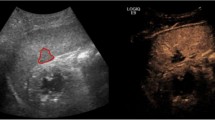
We collected data of patients admitted to our hospital from January 2006 to August 2008 for blunt splenic injury. During this period, 46 patients were admitted for splenic trauma, of whom 17 were treated surgically, 15 conservatively and 14 with percutaneous embolisation (13 men, mean age 44.8, mean injury severity score 18.5, six with grade IV and eight with contrast blush). Patients in shock were referred for laparotomy and splenectomy, whereas those who were haemodynamically stable or responsive to fluid resuscitation were further evaluated with computed tomography (CT). In the presence of imaging evidence of splenic injury ranging from grade I to grade III (n=15) a conservative approach was adopted, whereas haemodynamically unstable patients with grade V injury (n=17) were treated with splenectomy. Embolisation was performed in 14 patients with grade IV injury or in the event of contrast extravasation, regardless of injury grade. In patients with diffuse organ damage, we embolised the main splenic artery, whereas in the case of localised injury, embolisation was selective.
Results
Proximal embolization was required in eight cases and distal coil embolization in six. In 13 cases, we placed magnetic-resonance-compatible coils 4–6 mm in diameter; only one patient was treated with gel-foam injection. Immediate technical success was achieved in all cases. In 13/14 patients (92.9%), no periprocedural complications were observed, whereas the remaining patient underwent splenectomy within 24 h due to recurrent bleeding.
Conclusions
On the basis of our algorithm, it is possible to reach a quick decision on the most appropriate treatment for patients presenting with blunt abdominal trauma, and splenic artery embolization seems to offer a reliable option in those with high-grade splenic injury or active bleeding.
Riassunto
Obiettivo
Scopo del nostro lavoro è stato valutare i risultati della nostra esperienza sull’embolizzazione percutanea in pazienti con trauma splenico, sulla base di un algoritmo modificato.
Materiali e metodi
Abbiamo raccolto i dati dei pazienti con trauma della milza ammessi nel nostro centro da gennaio 2006 ad agosto 2008. In questo periodo sono stati ammessi 46 pazienti con lesione splenica posttraumatica, di cui 17 sono stati trattati chirurgicamente, 15 con trattamento conservativo e 14 con embolizzazione percutanea (13 maschi, età media 44,8, injury severity score [ISS] 18,5 circa, 6 con grado IV e 8 con stravaso di mezzo di contrasto). I pazienti in stato di shock sono stati immediatamente sottoposti a laparotomia e splenectomia, mentre quelli emodinamicamente stabili o responsivi alla somministrazione di fluidi sono stati valutati con TC. In base al dato strumentale, in 15 pazienti, con lesioni spleniche di grado I, II e III è stato considerato il trattamento conservativo, mentre 17 pazienti emodinamicamente instabili, con lesioni di V grado, sono stati sottoposti a splenectomia. L’embolizzazione è stata eseguita in 14 pazienti con lesioni spleniche di IV grado o in caso di stravaso di mezzo di contrasto indipendentemente dal grado della lesione. L’embolizzazione dell’arteria splenica principale è stata effettuata nei pazienti con danno d’organo diffuso, mentre in caso di lesioni localizzate, è stata eseguita l’occlusione selettiva del solo segmento splenico interessato.
Risultati
L’embolizzazione prossimale si è resa necessaria in 8 pazienti e quella distale in 6. In 13 casi sono state posizionate spirali RM compatibili con diametro variabile tra 4 e 6 mm; in un solo paziente sono state iniettate solo particelle riassorbibili. Il successo tecnico immediato è stato ottenuto in tutti i casi. In 13/14 casi (92,9%) non sono state osservate complicanze post-procedurali, mentre in un solo paziente, trattato con particelle riassorbibili, si è resa necessaria la splenectomia per recidiva di sanguinamento a 24 ore dall’embolizzazione.
Conclusioni
Sulla base del nostro algoritmo, è possibile una veloce decisione sul trattamento più opportuno delle lesioni spleniche post-traumatiche e l’embolizzazione percutanea sembra offrire un’affidabile opzione in pazienti con lesioni d’organo di grado elevato o con sanguinamento attivo.
Similar content being viewed by others

References/Bibliografia
Liu PP, Chou FF, Sheen-Chen SM et al (1994) Complications of splenectomy for splenic injury. Changgeng Yi Xue Za Zhi 17:125–130
William BM, Corazza GR (2007) Hyposplenism: a comprehensive review. Part I: basic concepts and causes. Hematology 12:1–13
Hansen K, Singer DB (2001) Asplenichyposplenic overwhelming sepsis: postsplenectomy sepsis revisited. Pediatr Dev Pathol 4:105–121
Diamond LK (1969) Splenectomy in childhood and the hazard of overwhelming infection. Pediatrics 43:886–889
Richardson JD (2005) Changes in the management of injuries to the liver and spleen. J Am Coll Surg 200:648–669
Peitzman AB, Heil B, Rivera L et al (2000) Blunt splenic injury in adults: Multi-Institutional Study of the Eastern Association for the Surgery of Trauma. J Trauma 49:177–187
Wasvary H, Howells G, Villalba M et al (1997) Nonoperative management of adult blunt splenic trauma: a 15-year experience. Am Surg 63:694–699
Smith JS Jr, Cooney RN, Mucha P Jr (1996) Nonoperative management of the ruptured spleen: a revalidation of criteria. Surgery 120:745–750
Longo WE, Baker CC, McMillen MA et al (1989) Nonoperative management of adult blunt splenic trauma. Criteria for successful outcome. Ann Surg 210:626–629
Cogbill TH, Moore EE, Jurkovich GJ et al (1989) Nonoperative management of blunt splenic trauma: a multicenter experience. J Trauma 29:1312–1317
Ochsner MG (2001) Factors of failure for nonoperative management of blunt liver and splenic injuries. World J Surg 25:1393–1396
Sclafani SJ, Weisberg A, Scalea TM et al (1991) Blunt splenic injuries: nonsurgical treatment with CT, arteriography, and transcatheter arterial embolization of the splenic artery. Radiology 181:189–196
Wu SC, Chow KC, Lee KH et al (2007) Early selective angioembolization improves success of nonoperative management of blunt splenic injury. Am Surg 73:897–902
Rajani RR, Claridge JA, Yowler CJ et al (2006) Improved outcome of adult blunt splenic injury: a cohort analysis. Surgery 140:625–631
Gaarder C, Dormagen JB, Eken T et al (2006) Nonoperative management of splenic injuries: improved results with angioembolization. J Trauma 61:192–198
Haan JM, Biffl W, Knudson MM et al (2004) Splenic embolization revisited: a multicenter review. J Trauma 56:542–547
Liu PP, Lee WC, Cheng YF et al (2004) Use of splenic artery embolization as an adjunct to nonsurgical management of blunt splenic injury. J Trauma 56:768–773
Dent D, Alsabrook G, Erickson BA et al (2004) Blunt splenic injuries: high nonoperative management rate can be achieved with selective embolization. J Trauma 56:1063–1067
Hagiwara A, Murata A, Matsuda T et al (2004) The usefulness of transcatheter arterial embolization for patients with blunt polytrauma showing transient response to fluid resuscitation. J Trauma 57:271–276
Bessoud B, Denys A, Calmes JM et al (2006) Nonoperative management of traumatic splenic injuries: is there a role for proximal splenic artery embolization? AJR Am J Roentgenol 186:779–785
Smith HE, Biffl WL, Majercik SD et al (2006) Splenic artery embolization: have we gone too far? J Trauma 61:541–544
Bessoud B, Denys A (2004) Main splenic artery embolization using coils in blunt splenic injuries: effects on the intrasplenic blood pressure. Eur Radiol 14:1718–1719
American College of Surgeons. Committee on Trauma (1997) Advanced Trauma Life Support Course for Physicians. American College of Surgeons, Chicago, pp 87–107
Moore EE, Cogbill TH, Jurkovich GJ et al (1995) Organ injury scaling: spleen and liver (1994 revision). J Trauma 38:323–324
Thompson BE, Munera F, Cohn SM et al (2006) Novel computed tomography scan scoring system predicts the need for intervention after splenic injury. J Trauma 60:1083–1086
Omert LA, Salyer D, Dunham CM et al (2001) Implications of the “contrast blush” finding on computed tomographic scan of the spleen in trauma. J Trauma 51:272–277
Valentino M, Ansaloni L, Catena F et al (2009) Contrast-enhanced ultrasonography in blunt abdominal trauma: consideration after 5 years of experience. Radiol Med 114:1080–1093
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Monaco, D., Franco, F., Marcato, C. et al. The role of arterial embolization in blunt splenic injury. Radiol med 116, 454–465 (2011). https://doi.org/10.1007/s11547-011-0624-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-011-0624-y