
Abstract
Background
Patients harboring concomitant epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) arrangements constitute a small subgroup of non-small-cell lung cancer (NSCLC) patients. The efficacy of EGFR tyrosine kinase inhibitors (TKIs) and the ALK-specific TKI crizotinib in these patients has not been well-established.
Objective
This study investigated the efficacy of targeted therapies in these patients compared with patients with EGFR or ALK alterations alone.
Methods
Patients were screened for EGFR mutation and ALK rearrangement at the Shanghai Chest Hospital (2011–2017). Progression-free survival (PFS), objective response rate (ORR), and overall survival (OS) were retrospectively analyzed.
Results
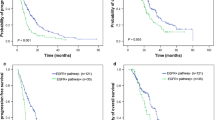
A total of 5816 patients were screened, and 26 patients were identified as having concomitant EGFR mutations and ALK rearrangements; 22 patients were eligible for survival analysis. Additionally, 95 EGFR-mutant patients and 60 ALK-rearranged patients were randomly selected for analysis. The ORR to EGFR TKIs was 63.2% (12/19) for EGFR/ALK co-altered patients and 62.1% (59/95) for EGFR-mutant patients (p = 0.93) with a median PFS of 10.3 and 11.4 months, respectively (hazard ratio [HR] 0.96; 95% confidence interval [CI] 0.59–1.57; p = 0.87). The ORR to crizotinib was 66.7% (8/12) for double-positive patients and 65.0% (39/60) for ALK-rearranged patients (p = 1.00), with a median PFS of 11.1 and 12.5 months, respectively (HR 1.39; 95% CI 0.69–2.80; p = 0.28). OS was 27.1, 36.2, and 36.8 months for EGFR-mutant, ALK-rearranged, and EGFR/ALK co-altered patients, respectively, and the EGFR/ALK co-existing subgroup tended to have a longer survival period than EGFR-mutant cohorts, though no statistical difference was found (p = 0.12). The median PFS of crizotinib as a sequential therapy after failure of EGFR TKIs was 15.0 months, which exhibited no statistically significant difference compared with the median PFS of ALK-altered patients who received crizotinib (p = 0.80).
Conclusions
Both first-generation EGFR TKIs and the ALK TKI crizotinib were effective in these patients. Sequential treatment with EGFR TKIs and crizotinib should be considered as a management option.



Similar content being viewed by others


References
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–32. https://doi.org/10.3322/caac.21338.
Chen W, Zheng R, Zeng H, Zhang S, He J. Annual report on status of cancer in China, 2011. Chin J Cancer Res Chung-kuo yen cheng yen chiu. 2015;27(1):2–12. https://doi.org/10.3978/j.issn.1000-9604.2015.01.06.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. https://doi.org/10.3322/caac.20107.
Kris MG, Johnson BE, Berry LD, Kwiatkowski DJ, Iafrate AJ, Wistuba II, et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA. 2014;311(19):1998–2006. https://doi.org/10.1001/jama.2014.3741.
Gainor JF, Varghese AM, Ou SH, Kabraji S, Awad MM, Katayama R, et al. ALK rearrangements are mutually exclusive with mutations in EGFR or KRAS: an analysis of 1,683 patients with non-small cell lung cancer. Clin Cancer Res. 2013;19(15):4273–81. https://doi.org/10.1158/1078-0432.ccr-13-0318.
Baldi L, Mengoli MC, Bisagni A, Banzi MC, Boni C, Rossi G. Concomitant EGFR mutation and ALK rearrangement in lung adenocarcinoma is more frequent than expected: report of a case and review of the literature with demonstration of genes alteration into the same tumor cells. Lung Cancer. 2014;86(2):291–5. https://doi.org/10.1016/j.lungcan.2014.09.011.
Kuo YW, Wu SG, Ho CC, Shih JY. Good response to gefitinib in lung adenocarcinoma harboring coexisting EML4-ALK fusion gene and EGFR mutation. J Thorac Oncol. 2010;5(12):2039–40. https://doi.org/10.1097/JTO.0b013e3181f43274.
Lo Russo G, Imbimbo M, Corrao G, Proto C, Signorelli D, Vitali M, et al. Concomitant EML4-ALK rearrangement and EGFR mutation in non-small cell lung cancer patients: a literature review of 100 cases. Oncotarget. 2017;8(35):59889–900. https://doi.org/10.18632/oncotarget.17431.
Lou NN, Zhang XC, Chen HJ, Zhou Q, Yan LX, Xie Z, et al. Clinical outcomes of advanced non-small-cell lung cancer patients with EGFR mutation, ALK rearrangement and EGFR/ALK co-alterations. Oncotarget. 2016;7(40):65185–95. https://doi.org/10.18632/oncotarget.11218.
Popat S, de Vieira Araujo A, Min T, Swansbury J, Dainton M, Wotherspoon A, et al. Lung adenocarcinoma with concurrent exon 19 EGFR mutation and ALK rearrangement responding to erlotinib. J Thorac Oncol. 2011;6(11):1962–3. https://doi.org/10.1097/jto.0b013e31822eec5e.
Sahnane N, Frattini M, Bernasconi B, Zappa F, Schiavone G, Wannesson L, et al. EGFR and KRAS mutations in ALK-positive lung adenocarcinomas: biological and clinical effect. Clin Lung Cancer. 2016;17(1):56–61. https://doi.org/10.1016/j.cllc.2015.08.001.
Sweis RF, Thomas S, Bank B, Fishkin P, Mooney C, Salgia R. Concurrent EGFR mutation and ALK translocation in non-small cell lung cancer. Cureus. 2016;8(2):e513. https://doi.org/10.7759/cureus.513.
Tanaka H, Hayashi A, Morimoto T, Taima K, Tanaka Y, Shimada M, et al. A case of lung adenocarcinoma harboring EGFR mutation and EML4-ALK fusion gene. BMC Cancer. 2012;12:558. https://doi.org/10.1186/1471-2407-12-558.
Tiseo M, Gelsomino F, Boggiani D, Bortesi B, Bartolotti M, Bozzetti C, et al. EGFR and EML4-ALK gene mutations in NSCLC: a case report of erlotinib-resistant patient with both concomitant mutations. Lung Cancer. 2011;71(2):241–3. https://doi.org/10.1016/j.lungcan.2010.11.014.
Won JK, Keam B, Koh J, Cho HJ, Jeon YK, Kim TM, et al. Concomitant ALK translocation and EGFR mutation in lung cancer: a comparison of direct sequencing and sensitive assays and the impact on responsiveness to tyrosine kinase inhibitor. Ann Oncol. 2015;26(2):348–54. https://doi.org/10.1093/annonc/mdu530.
Yang JJ, Zhang XC, Su J, Xu CR, Zhou Q, Tian HX, et al. Lung cancers with concomitant EGFR mutations and ALK rearrangements: diverse responses to EGFR-TKI and crizotinib in relation to diverse receptors phosphorylation. Clin Cancer Res. 2014;20(5):1383–92. https://doi.org/10.1158/1078-0432.ccr-13-0699.
Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–57. https://doi.org/10.1056/NEJMoa0810699.
Shi YK, Wang L, Han BH, Li W, Yu P, Liu YP, et al. First-line icotinib versus cisplatin/pemetrexed plus pemetrexed maintenance therapy for patients with advanced EGFR mutation-positive lung adenocarcinoma (CONVINCE): a phase 3, open-label, randomized study. Ann Oncol. 2017;28(10):2443–50. https://doi.org/10.1093/annonc/mdx359.
Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12(8):735–42. https://doi.org/10.1016/s1470-2045(11)70184-x.
Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. 2014;371(23):2167–77. https://doi.org/10.1056/NEJMoa1408440.
Lee JK, Kim TM, Koh Y, Lee SH, Kim DW, Jeon YK, et al. Differential sensitivities to tyrosine kinase inhibitors in NSCLC harboring EGFR mutation and ALK translocation. Lung Cancer. 2012;77(2):460–3. https://doi.org/10.1016/j.lungcan.2012.04.012.
Kim HJ, Lee KY, Kim YC, Kim KS, Lee SY, Jang TW, et al. Detection and comparison of peptide nucleic acid-mediated real-time polymerase chain reaction clamping and direct gene sequencing for epidermal growth factor receptor mutations in patients with non-small cell lung cancer. Lung Cancer. 2012;75(3):321–5. https://doi.org/10.1016/j.lungcan.2011.08.005.
Newton CR, Graham A, Heptinstall LE, Powell SJ, Summers C, Kalsheker N, et al. Analysis of any point mutation in DNA. The amplification refractory mutation system (ARMS). Nucleic Acids Res. 1989;17(7):2503–16.
Mino-Kenudson M, Chirieac LR, Law K, Hornick JL, Lindeman N, Mark EJ, et al. A novel, highly sensitive antibody allows for the routine detection of ALK-rearranged lung adenocarcinomas by standard immunohistochemistry. Clin Cancer Res. 2010;16(5):1561–71. https://doi.org/10.1158/1078-0432.ccr-09-2845.
Yi ES, Boland JM, Maleszewski JJ, Roden AC, Oliveira AM, Aubry MC, et al. Correlation of IHC and FISH for ALK gene rearrangement in non-small cell lung carcinoma: IHC score algorithm for FISH. J Thorac Oncol. 2011;6(3):459–65. https://doi.org/10.1097/JTO.0b013e318209edb9.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47. https://doi.org/10.1016/j.ejca.2008.10.026.
Lindeman NI, Cagle PT, Beasley MB, Chitale DA, Dacic S, Giaccone G, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Mol Diagn. 2013;15(4):415–53. https://doi.org/10.1016/j.jmoldx.2013.03.001.
Ulivi P, Chiadini E, Dazzi C, Dubini A, Costantini M, Medri L, et al. Nonsquamous, non-small-cell lung cancer patients who carry a double mutation of EGFR, EML4-ALK or KRAS: frequency, clinical-pathological characteristics, and response to therapy. Clin Lung Cancer. 2016;17(5):384–90. https://doi.org/10.1016/j.cllc.2015.11.004.
Cai W, Lin D, Wu C, Li X, Zhao C, Zheng L, et al. Intratumoral heterogeneity of ALK-rearranged and ALK/EGFR coaltered lung adenocarcinoma. J Clin Oncol. 2015;33(32):3701–9. https://doi.org/10.1200/jco.2014.58.8293.
Sasaki T, Koivunen J, Ogino A, Yanagita M, Nikiforow S, Zheng W, et al. A novel ALK secondary mutation and EGFR signaling cause resistance to ALK kinase inhibitors. Cancer Res. 2011;71(18):6051–60. https://doi.org/10.1158/0008-5472.can-11-1340.
Acknowledgements
The authors acknowledge all the patients and their families for their contributions to this study. No writing assistance was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No external funding was used in the preparation of this manuscript.
Conflict of interest
Yiming Zhao, Shuyuan Wang, Bo Zhang, Rong Qiao, Jianlin Xu, Lele Zhang, Yanwei Zhang and Baohui Han have no conflicts of interest that might be relevant to the contents of this manuscript.
Rights and permissions
About this article

Cite this article
Zhao, Y., Wang, S., Zhang, B. et al. Clinical Management of Non-Small Cell Lung Cancer with Concomitant EGFR Mutations and ALK Rearrangements: Efficacy of EGFR Tyrosine Kinase Inhibitors and Crizotinib. Targ Oncol 14, 169–178 (2019). https://doi.org/10.1007/s11523-019-00628-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-019-00628-6