
Abstract
Fear is a central emotional response to imminent threats such as the coronavirus-19 disease (COVID-19). The Fear of COVID-19 Scale (FCV-19S) assesses the severity of fear towards COVID-19. The present study examined the psychometric properties of the Arabic version of the FCV-19S. Using a forward-backward translation, the FCV-19S was translated into Arabic. An online survey using the Arabic versions of FCV-19S and the Hospital Anxiety and Depression Scale (HADS) was administered. Reliability and concurrent and confirmatory validity were examined. The dataset consisted of 693 Saudi participants. The internal consistency of the Arabic FCV-19S was satisfactory (α = .88), with sound concurrent validity indicated by significant and positive correlations with HADS (r = .66). The unidimensional structure of the FCV-19S was confirmed. The Arabic version of the FCV-19S is psychometrically robust and can be used in research assessing the psychological impact of COVID-19 among a Saudi adult population.
Similar content being viewed by others


The coronavirus 2019 disease (COVID-19) outbreak in December 2019, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a major global health crisis (Lipsitch et al. 2020). Declared by the World Health Organization as a global pandemic on March 11th, 2020 (Cucinotta and Vanelli 2020), COVID-19 had spread to more than 212 countries and territories since December 2019 until the time of writing this paper. Thus far (as of May 11th, 2020), crude data shows that there are more than four million confirmed cases and 282,872 deaths attributed to COVID-19 worldwide (Dong et al. 2020). In Saudi Arabia, the number of confirmed cases has exceeded 39,000 with 246 deaths as of May 11th, 2020 (Saudi Center for Disease Prevention and Control 2020).
While efforts are focused on developing and testing effective treatment options, a number of public health measures have been utilized to help slow the spread of the virus including physical distancing, self-isolation, and handwashing (World Health Organization 2020). Governments around the world have also taken unprecedented measures such as border control, lockdown, and contact tracing to contain the COVID-19 outbreak, all of which coming at significant economic cost (Al-Awadhi et al. 2020; Laing 2020).
The COVID-19 pandemic itself as well as the public health measures (e.g., lockdown) and their subsequent consequences (e.g., job losses, financial insecurities, and disruption to day-to-day activities) are likely to have a major adverse impact on mental health and well-being (Galea et al. 2020). Indeed, there are growing concerns about the psychological impact of the COVID-19 pandemic (Holmes et al. 2020; Van Bavel et al. 2020), with available research showing that the COVID-19 pandemic has profound psychological effects on general populations (Rajkumar 2020; Roy et al. 2020; Wang et al. 2020; Zhang et al. 2020), people with COVID-19 mild symptoms (Xiao et al. 2020) and healthcare professionals (Kang et al. 2020; Lu et al. 2020; Rajkumar 2020; Tan et al. 2020). For example, a study of 52,730 participants in China found that almost 35% of the sample reported experiencing psychological distress (Qiu et al. 2020). Similarly, another study of 7236 participants found that anxiety and depression symptoms were widely prevalent (i.e., 35% and 20%, respectively) (Huang and Zhao 2020). Healthcare professionals are also affected, with studies reporting psychological distress including stress, anxiety, depression, posttraumatic anxiety disorder (Jizheng et al. 2020; Tan et al. 2020), poor quality of sleep (Huang and Zhao 2020), and insomnia (Lai et al. 2020).
The COVID-19 pandemic may also exacerbate poor psychological health, loneliness, and social isolation in particular (Holmes et al. 2020), which are strongly associated with increased anxiety, depression, and self-harm (Dsouza et al. 2020; Matthews et al. 2019). Earlier research has shown that poor psychological health is associated with the development of physical medical conditions. For example, loneliness and social isolation were associated with increased risk of coronary heart disease, stroke (Valtorta et al. 2016), suicidal ideation and suicide attempts (Calati et al. 2019), and premature death (Elovainio et al. 2017; Holt-Lunstad et al. 2015).
Fear is a central emotional response to imminent threats such as COVID-19 (Van Bavel et al. 2020). In the extended parallel process model, fear is defined as psychological arousal and negative emotional response stimulated by overestimation of perceived threat, coupled with an underestimation of the perceived benefits from action as well as low self-efficacy (Witte 1992). While strong fear levels coupled with high self-efficacy have been shown to positively affect adaptive behavioral changes, low fear and self-efficacy levels were associated with engaging in avoidant behaviors (Witte and Allen 2000). For example, in cancer screening research, moderate levels of fear combined with high self-efficacy tended to motivate individuals to perform screening, whereas low and high levels of fear resulted in low levels of motivation to uptake screening and promotes engagement in avoidance behavior (Champion et al. 2004, 2008).
In line with previous research during viral epidemics (severe acute respiratory syndrome (Reynolds et al. 2008) and the Middle East respiratory syndrome-corona virus (Bukhari et al. 2016)), COVID-19-related research found evidence of increasing levels of fear worldwide (Knipe et al. 2020). This increase in fear levels was also evident among frontline medical staff (Lu et al. 2020). Excessive fear of COVID-19 (e.g., being infected or infecting others) may worsen anxiety symptoms (which is, by definition, excessive fear and avoidance) (Shin and Liberzon 2010) in people with pre-existing psychological disorders and could create psychological distress in the general population. Excessive fear of COVID-19 has also been associated with cases of suicide in Bangladesh (Mamun and Griffiths 2020) and India (Goyal et al. 2020).
On the other hand, fear could act as a motivator for behavioral change in the COVID-19 context (Harper et al. 2020; Pakpour and Griffiths 2020), especially when coupled with high self-efficacy and perceived benefits (Witte and Allen 2000). A recent study showed that fear of COVID-19 was a significant predictor of improved social distancing and hand hygiene, suggesting that fear plays an important role in compliance with COVID-19 related public health measures (Harper et al. 2020).
Due to the novel nature of COVID-19 and the psychological distress associated with it, it is argued that researchers should assess fear of COVID-19 to help determine whether prevention and support programs are needed, and if so, which groups of people to target (Pakpour and Griffiths 2020). Ahorsu and colleagues recently developed the Fear of COVID-19 Scale (FCV-19S), a self-report unidimensional scale that measures the severity of fear of COVID-19 after extensive literature search of all available fear measures (Ahorsu et al. 2020). The FCV-19S is a 7-item scale that is easy to administer and has shown satisfactory psychometric properties (Ahorsu et al. 2020). However, before the scale can be used in other populations and cultures, it is recommended that the psychometric properties of the scale in the target language are examined (Sousa and Rojjanasrirat 2011).
Aim of the Study
In the present study, we report reliability qualities, concurrent validity, and construct (confirmatory) validity of the Arabic version of the FCV-19S.
Methods
Participants
Data reported in this paper were part of a larger ongoing web-based study in Saudi Arabia, which is looking at understanding people’s awareness, attitudes, emotions, beliefs, and behaviors about COVID-19. Eligible participants were members of the general Saudi population who were at least 18 years of age and spoke Arabic as their first language. To validate the Arabic version of the FCV-19S, a dataset comprising 639 participants was used.
Procedure
Participants were recruited using an anonymous online survey and a snowball sampling strategy. Study announcements, containing brief information about the study and a web-page link to the study, were shared via email (to personal and professional networks), and posted on LinkedIn and other popular social media websites including Twitter and Facebook. The online survey was administered by Google Forms to ensure a wide reach and easy access. Participants were asked to kindly share the survey with their personal and professional networks.
After agreeing to complete the survey, participants provided demographic information and completed a battery of measures including the FCV-19S. Answers to all questionnaire items were required, and respondents were able to submit their responses only if all questions were answered. Data reported in this study were collected between the 11th and 20th of April 2020. Participation was voluntary, and all participants gave electronic informed consent and received no compensation for their participation. No identifying information were collected to protect the participants’ anonymity. This study was reviewed and approved by Taif University Research Ethics Committee (IRB 41–00155).
Adaptation of FCV-19S into Arabic
In line with established protocols for cross-cultural adaptation, the original FCV-19S was translated into Arabic using a forward-backward translation technique (Alyami et al. 2019; Henning et al. 2020). First, the FCV-19S was translated into Arabic by an independent professional medical translator who is fluent in English and Arabic. Second, one of the authors, who is fluent in English and Arabic, reviewed the provisional Arabic translation and discussed any anomalies with the independent translator. Third, the approved Arabic translation draft of the scale was then back translated into English by another author who at this time was unfamiliar with the original English scale. Both the forward and backward translations of the scale were then compared for equivalence and checked for cultural appropriateness among the authors. The approved Arabic translation was then piloted with 20 people recruited on Twitter to examine the scale readability and potential ambiguity. There were no apparent problems, and no further changes were deemed necessary. The final Arabic version of the FCV-19S can be found in the Appendix.
Measures
Participants reported their age, sex, marital status, education level, employment status, monthly income, and region. A battery of measures was administered which included the Arabic versions of the FCV-19S and Hospital Anxiety and Depression Scale (HADS).
Fear of COVID-19
The FCV-19S is a unidimensional scale that measures one’s fear levels of COVID-19 (Ahorsu et al. 2020). It consists of 7 items (e.g., items 7 states “My heart races or palpitates when I think about getting coronavirus-19”) and is scored on a 5-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree). A total score is calculated by summing all item scores with a possible total score ranging between 7 and 35. Higher scores indicate greater levels of fear of COVID-19. The scale has shown robust psychometric properties including high internal consistency (α = .82) (Ahorsu et al. 2020). The scale is also now available in three languages including Italian (Soraci et al. 2020), Bangla (Sakib et al. 2020), and Turkish (Satici et al. 2020).
Psychological Distress
Psychological distress was assessed using the HADS (Zigmond and Snaith 1983). The HADS consists of a total of 14 items, 7 items for the anxiety subscale (HADS-A, e.g., item 1 states “I feel tense or ‘wound up’”) and 7 items for the depression subscale (HADS-D, e.g., items 10 states “I have lost interest in my appearance”). Each item is rated on a 4-point scale. After reverse scoring six items (2 for anxiety and 4 for depression), relevant item scores are added to produce HADS-A and HADS-D total scores, with possible total scores ranging from 0 to 21 for each subscale. Additionally, an overall total score (HADS-T) can also be calculated by summing all items (0–42 range), with higher scores indicating greater levels of psychological distress (Zigmond and Snaith 1983). The HADS has demonstrated satisfactory psychometric properties in different patient groups as well as in general populations (Bjelland et al. 2002; Mykletun et al. 2001). The Arabic version of the HADS has also shown acceptable psychometric properties (Terkawi et al. 2017). Internal consistency in the current study was α = .86 for the HADS-A, α = .80 for the HADS-D, and α = .90 for the whole scale.
Statistical Analysis
Descriptive statistics were used to report the sample characteristics. Skewness, kurtosis, and distributions of responses were analyzed with respect to each item. Internal consistency was assessed by Cronbach alpha coefficients (α), inter-item correlations and corrected item-total correlations. A Cronbach’s α of .70 or higher indicates acceptable reliability (DeVellis 2016; Nunnally and Bernstein 1994). Each item was also assessed in terms of its impact on the overall alpha correlation coefficient. Inter-item correlations and corrected item-total correlations between .30 and .70 suggest medium to strong associations between items (Ferketich 1991). Concurrent validity was assessed by comparing the Pearson correlations between the FCV-19S and HADS-D, HADS-A, and HADS-T. These analyses were conducted using the IBM SPSS Statistics v 26 software.
To investigate the proposed theoretical domain structure, a confirmatory factor analysis (CFA) was conducted on the FCV-19S dataset. Factor structure was conducted using the LISREL v.8.80 software. As the data were ordinal, a diagonally weighted least squares method of estimation with polychoric correlations was most appropriate (Flora and Curran 2004). Goodness of fit was assessed according to the following criteria: root mean square error of approximation (RMSEA ≤ .06); comparative fit index (CFI > .90 or more desirably ≥ .95); and standardized root mean square residual (SRMR ≤ .08) (Lei and Wu 2007).
Results
Table 1 shows sample characteristics. The dataset included 639 individual complete responses. The mean age was 34.75 years (SD 11.80). Overall, more than half of the participants were males (57.9%), married (58.4%), has a university qualification (70.0%), employed (50.2%), and earned 9999 Saudi Riyal and less a month (52.0%). Participants were from all regions, with the Northern region being the least represented in this dataset.
The measures of central tendency, internal consistency, skewness, kurtosis, and distributions of responses of each item (Tables 2 and 3) provided a good description of the item distributions and their reliability as used in the COVID-19 measure. Byrne and Campbell stated that a normal distribution can be demonstrated when values of skewness and kurtosis are close to zero (between − 1.5 and + 1.5) (Byrne and Campbell 1999). The values presented in Table 2 suggest that items 3, 6, and 7 are unlikely to be normally distributed, although all items were found to be reliable. The distributions in Table 4 indicate that most respondents strongly disagreed with the item 3, 6, and 7 statements.
Internal Consistency and Concurrent Validity
The internal consistency of the Arabic FCV-19S was good (α = .88). The inter-item correlations ranged between 0.35 and 0.66, and the corrected item-total correlations of each item ranged between 0.57 and 0.74 indicating that the Arabic FCV-19S has adequate internal consistency (Table 4). Concurrent validity was supported by the significant correlations with the psychological distress as assessed by the HADS. Fear of COVID-19 was significantly correlated with HADS-D (r = .56, p < .001), HADS-A (r = .66, p < .001), and HADS-T (r = .66, p < .001).
Factor Analysis of the Arabic FCV-19S
Model 1 of the CFA denotes the baseline model, which tested a unidimensional solution with all seven items and no error variances correlated. CFI and SRMR indicated that the fit was already excellent at this stage, but RMSEA was still clearly above the criterion of 0.06 (Table 5). The pattern of modification indices and inter-item correlations suggested the presence of notable error co-variance within the cluster of item 3 (“My hands become clammy when I think about coronavirus-19”), item 6 (“I cannot sleep because I am worrying about coronoavirsu-19”), and item 7 (“My heart races or palpitates when I think about getting coronavirus-19”). When the error variance of these items was correlated in model 2, RMSEA decreased substantially, although it was still above the required cut-off value.
Furthermore, modification indices strongly suggested that the error variances of item 1 (“I am most afraid of coronavirus-19”) and item 2 (“It makes me uncomfortable to think about coronavirus-19”) be correlated, which was implemented in the subsequent step. The resulting solution (model 3) presented with CFI and SRMR clearly exceeding their required cut-off values, and RMSEA was now also below its cut-off of 0.06 (Table 5). Figures 1 and 2 present an overview of the factor solution for models 1 and 3, respectively. Shown there are the factor loadings. These were slightly higher for model 1 (range 0.73 to 0.86) than for model 3 (range 0.62 to 0.84), but in both cases, factor loadings confirm the strong psychometric performance of the scale.

Baseline model with no covariances correlated

Model 3 with covariances between q1 and q2, q3 and q6, q3 and q7, and q6 and q7
Discussion
Using a sample of Saudi adults, the present study aimed to evaluate the psychometric properties of the Arabic version of the FCV-19S to ensure this was a reliable and a valid measure that can be used to assess the severity of fear of COVID-19 among the Saudi general adult population. The findings showed that the Arabic FCV-19S had a unidimensional structure, good internal consistency, good concurrent validity, and acceptable construct validity.
Overall, our findings were similar to previous research using the FCV-19S. Internal consistency of the Arabic FCV-19S was .88, which is marginally higher than that reported for the original scale (α = .82) (Ahorsu et al. 2020), and Italian (α = .87) (Soraci et al. 2020), Bangla (α = .87) (Sakib et al. 2020), and Turkish (α = .85) versions (Satici et al. 2020). Concurrent validity analysis showed significant positive correlations with anxiety and depression as assessed by the HADS, and this was also consistent with previous findings (Ahorsu et al. 2020; Sakib et al. 2020; Satici et al. 2020; Soraci et al. 2020).
Results of the CFA provided evidence for the unidimensional structure of the Arabic FCV-19S. Factor loadings were all significant and strong (range 0.62 to 0.84), comparable with other versions of the scale (.68 to .90 for the Italian version and .72 to .80 for the Bangla version) (Sakib et al. 2020; Soraci et al. 2020). However, items 3, 6, and 7 had lower mean values compared with the rest of the items, indicating that respondents tended to strongly disagree with these statements. This was also the case among Italian (Soraci et al. 2020), Turkish (Satici et al. 2020) and Bangladeshi respondents (Sakib et al. 2020) but not Iranian respondents (Ahorsu et al. 2020). Item 3, 6, and 7 have shared meaning in that they all refer to somatic aspects related to COVID-19 fear (clammy hands, lack of sleep, heart racing). However, there was not enough evidence for these items to form a separate factor, as inter-item correlations did not indicate a clearly distinguishable factor, and the misfit in model 1 could be adequately resolved by correlating shared error variance between these items.
The only other remaining instance of notable error co-variance was for items 1 and 2. Both items also have some shared meaning in comparison with the rest, as items 1 and 2 are both general questions about being afraid of COVID-19 or feeling uncomfortable when thinking about COVID-19. This is in contrast to the other items that contain specific aspects, such as the somatic elements of the cluster 3, 6, and 7, losing one’s life (item 4), or becoming anxious when watching the news (item 5).
Recent studies using the FCV-19S showed that fear of COVID-19 was negatively associated with life satisfaction (r = − .20, p < .001) and this relationship was mediated by depression, anxiety, and stress (Satici et al. 2020). Another study reported that greater fear of COVID-19 was associated reduced physical and environmental quality of life (which is unsurprising given that people are in lockdown) and improved social distancing and hand hygiene practices, suggesting that fear plays an important role in motivating people to comply with COVID-19-related recommended health behaviors (Harper et al. 2020).
Given the significant correlations between fear of COVID-19 and anxiety and depression, longitudinal studies are warranted to determine the direction of this relationship. Future research could also investigate how fear of COVID-19 affects the extent to which people practice social distancing, hand washing, and other public health measures within COVID-19 context. Our findings should be viewed in light of some limitations. The snowball sampling method used during the lockdown and quarantine measures, put in place by the Government, may have introduced selection bias, where only those who received the study link had the chance to participate. Moreover, although recruitment of participants through LinkedIn was low compared with other social media platforms, LinkedIn could be considered as a niche social media platform. This might have produced a subsample of biased participants in terms of socio-demographics. In conclusion, the results of the present study demonstrated that the Arabic FCV-19S has a unidimensional structure with robust psychometric properties and hence can be used in research assessing the psychological impact of COVID-19 among the Saudi adult population.
References
Ahorsu, D. K., Lin, C.-Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The fear of COVID-19 scale: development and initial validation. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00270-8.
Al-Awadhi, A. M., Alsaifi, K., Al-Awadhi, A., & Alhammadi, S. (2020). Death and contagious infectious diseases: impact of the COVID-19 virus on stock market returns. Journal of Behavioral and Experimental Finance, 27, 100326. https://doi.org/10.1016/j.jbef.2020.100326.
Alyami, M., Al-Sharef, A., Al-Aseri, M., & Henning, M. (2019). Mammography self-efficacy scale and breast cancer fear scale: psychometric properties of the Arabic versions among Saudi women. Cancer Nursing. https://doi.org/10.1097/NCC.0000000000000767.
Bjelland, I., Dahl, A. A., Haug, T. T., & Neckelmann, D. (2002). The validity of the hospital anxiety and depression scale: an updated literature review. Journal of Psychosomatic Research, 52(2), 69–77. https://doi.org/10.1016/S0022-3999(01)00296-3.
Bukhari, E. E., Temsah, M. H., Aleyadhy, A. A., Alrabiaa, A. A., Alhboob, A. A., Jamal, A. A., & Binsaeed, A. A. (2016). Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak perceptions of risk and stress evaluation in nurses. Journal of Infection in Developing Countries, 10(8), 845–850. https://doi.org/10.3855/jidc.6925.
Byrne, B. M., & Campbell, T. L. (1999). Cross-cultural comparisons and the presumption of equivalent measurement and theoretical structure: a look beneath the surface. Journal of Cross-Cultural Psychology, 30(5), 555–574. https://doi.org/10.1177/0022022199030005001.
Calati, R., Ferrari, C., Brittner, M., Oasi, O., Olié, E., Carvalho, A. F., & Courtet, P. (2019). Suicidal thoughts and behaviors and social isolation: a narrative review of the literature. Journal of Affective Disorders, 245, 653–667. https://doi.org/10.1016/j.jad.2018.11.022.
Champion, V. L., Skinner, C. S., Menon, U., Rawl, S., Giesler, R. B., Monahan, P., & Daggy, J. (2004). A breast cancer fear scale: psychometric development. Journal of Health Psychology, 9(6), 753–762. https://doi.org/10.1177/1359105304045383.
Champion, V. L., Monahan, P. O., Springston, J. K., Russell, K., Zollinger, T. W., Saywell, R. M., & Maraj, M. (2008). Measuring mammography and breast cancer beliefs in African American women. Journal of Health Psychology, 13(6), 827–837. https://doi.org/10.1177/1359105308093867.
Cucinotta, D., & Vanelli, M. (2020). WHO declares COVID-19 a pandemic. Acta Bio-Medica: Atenei Parmensis, 91(1), 157–160. https://doi.org/10.23750/abm.v91i1.9397.
DeVellis, R. F. (2016). Scale development: theory and applications (4th ed.). SAGE.
Dong, E., Du, H., & Gardner, L. (2020). An interactive web-based dashboard to track COVID-19 in real time. The Lancet Infectious Diseases, 20(5), 533–534. https://doi.org/10.1016/S1473-3099(20)30120-1.
Dsouza, D. D., Quadros, S., Hyderabadwala, Z. J., & Mamun, M. A. (2020). Aggregated COVID-19 suicide incidences in India: fear of COVID-19 infection is the prominent causative factor. PsyArVix Preprints. https://doi.org/10.31234/osf.io/7xa4b.
Elovainio, M., Hakulinen, C., Pulkki-Råback, L., Virtanen, M., Josefsson, K., Jokela, M., Vahtera, J., & Kivimäki, M. (2017). Contribution of risk factors to excess mortality in isolated and lonely individuals: an analysis of data from the UK Biobank cohort study. The Lancet Public Health, 2(6), e260–e266. https://doi.org/10.1016/S2468-2667(17)30075-0.
Ferketich, S. (1991). Focus on psychometrics. Aspects of item analysis. Research in Nursing & Health, 14(2), 165–168. https://doi.org/10.1002/nur.4770140211.
Flora, D. B., & Curran, P. J. (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9(4), 466–491. https://doi.org/10.1037/1082-989X.9.4.466.
Galea, S., Merchant, R. M., & Lurie, N. (2020). The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Internal Medicine. https://doi.org/10.1001/jamainternmed.2020.1562.
Goyal, K., Chauhan, P., Chhikara, K., Gupta, P., & Singh, M. P. (2020). Fear of COVID 2019: first suicidal case in India! Asian Journal of Psychiatry, 49, 101989. https://doi.org/10.1016/j.ajp.2020.101989.
Harper, C. A., Satchell, L. P., Fido, D., & Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID-19 pandemic. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00281-5.
Henning, M., Alyami, M., Melyani, Z., Alyami, H., & Al Mansour, A. (2020). Development of the cross-cultural academic integrity questionnaire—version 3 (CCAIQ-3). Journal of Academic Ethics, 18(1), 35–53. https://doi.org/10.1007/s10805-019-09350-4.
Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., Ballard, C., Christensen, H., Silver, R. C., Everall, I., Ford, T., John, A., Kabir, T., King, K., Madan, I., Michie, S., Przybylski, A. K., Shafran, R., Sweeney, A., et al. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet Psychiatry. https://doi.org/10.1016/S2215-0366(20)30168-1.
Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives on Psychological Science, 10(2), 227–237. https://doi.org/10.1177/1745691614568352.
Huang, Y., & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: a web-based cross-sectional survey. MedRxiv. https://doi.org/10.1101/2020.02.19.20025395.
Jizheng, H., Mingfeng, H., Tengda, L., Ake, R., & Xiaoping, Z. (2020). A survey of mental health of medical staff in new-type coronavirus pneumonia hospitals. Chinese Journal of Industrial Hygiene and Occupational Diseases, 38, Article 00. https://doi.org/10.3760/cma.j.cn121094-20200219-00063.
Kang, L., Ma, S., Chen, M., Yang, J., Wang, Y., Li, R., Yao, L., Bai, H., Cai, Z., Xiang Yang, B., Hu, S., Zhang, K., Wang, G., Ma, C., & Liu, Z. (2020). Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain, Behavior, and Immunity. https://doi.org/10.1016/j.bbi.2020.03.028.
Knipe, D., Evans, H., Marchant, A., Gunnell, D., & John, A. (2020). Mapping population mental health concerns related to COVID-19 and the consequences of physical distancing: a Google trends analysis. Wellcome Open Research, 5, 82–92. https://doi.org/10.12688/wellcomeopenres.15870.1.
Lai, J., Ma, S., Wang, Y., Cai, Z., Hu, J., Wei, N., Wu, J., Du, H., Chen, T., Li, R., Tan, H., Kang, L., Yao, L., Huang, M., Wang, H., Wang, G., Liu, Z., & Hu, S. (2020). Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open, 3(3), e203976. https://doi.org/10.1001/jamanetworkopen.2020.3976.
Laing, T. (2020). The economic impact of the coronavirus 2019 (Covid-2019): implications for the mining industry. The Extractive Industries and Society. https://doi.org/10.1016/j.exis.2020.04.003.
Lei, P.-W., & Wu, Q. (2007). Introduction to structural equation modeling: issues and practical considerations. Educational Measurement: Issues and Practice, 26(3), 33–43. https://doi.org/10.1111/j.1745-3992.2007.00099.x.
Lipsitch, M., Swerdlow, D. L., & Finelli, L. (2020). Defining the epidemiology of Covid-19—studies needed. New England Journal of Medicine, 382(13), 1194–1196. https://doi.org/10.1056/NEJMp2002125.
Lu, W., Wang, H., Lin, Y., & Li, L. (2020). Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Research, 288, 112936. https://doi.org/10.1016/j.psychres.2020.112936.
Mamun, M. A., & Griffiths, M. D. (2020). First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: possible suicide prevention strategies. Asian Journal of Psychiatry, 51, 102073. https://doi.org/10.1016/j.ajp.2020.102073.
Matthews, T., Danese, A., Caspi, A., Fisher, H. L., Goldman-Mellor, S., Kepa, A., Moffitt, T. E., Odgers, C. L., & Arseneault, L. (2019). Lonely young adults in modern Britain: findings from an epidemiological cohort study. Psychological Medicine, 49(2), 268–277. https://doi.org/10.1017/S0033291718000788.
Mykletun, A., Stordal, E., & Dahl, A. A. (2001). Hospital Anxiety and Depression (HAD) scale: Factor structure, item analyses and internal consistency in a large population. The British Journal of Psychiatry, 179(6), 540–544. https://doi.org/10.1192/bjp.179.6.540.
Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory (3rd ed.). McGraw-Hill.
Pakpour, A. H., & Griffiths, M. D. (2020). The fear of COVID-19 and its role in preventive behaviors. Journal of Concurrent Disorders. https://concurrentdisorders.ca/2020/04/03/the-fear-of-covid-19-and-its-role-in-preventive-behaviors/.
Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B., & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General Psychiatry, 33(2), e100213. https://doi.org/10.1136/gpsych-2020-100213.
Rajkumar, R. P. (2020). COVID-19 and mental health: a review of the existing literature. Asian Journal of Psychiatry, 52, 102066. https://doi.org/10.1016/j.ajp.2020.102066.
Reynolds, D. L., Garay, J. R., Deamond, S. L., Moran, M. K., Gold, W., & Styra, R. (2008). Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiology & Infection, 136(7), 997–1007. https://doi.org/10.1017/S0950268807009156.
Roy, D., Tripathy, S., Kar, S. K., Sharma, N., Verma, S. K., & Kaushal, V. (2020). Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian Journal of Psychiatry, 51, 102083. https://doi.org/10.1016/j.ajp.2020.102083.
Sakib, N., Bhuiyan, A. K. M. I., Hossain, S., Al Mamun, F., Hosen, I., Abdullah, A. H., Sarker, M. A., Mohiuddin, M. S., Rayhan, I., Hossain, M., Sikder, M. T., Gozal, D., Muhit, M., Islam, S. M. S., Griffiths, M. D., Pakpour, A. H., & Mamun, M. A. (2020). Psychometric validation of the Bangla Fear of COVID-19 Scale: confirmatory factor analysis and Rasch analysis. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00289-x.
Satici, B., Gocet-Tekin, E., Deniz, M. E., & Satici, S. A. (2020). Adaptation of the Fear of COVID-19 Scale: its association with psychological distress and life satisfaction in Turkey. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00294-0.
Saudi Center for Disease Prevention and Control. (2020). Saudi Center for Disease Prevention and Control [Gov]. https://covid19.cdc.gov.sa/
Shin, L. M., & Liberzon, I. (2010). The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology, 35(1), 169–191. https://doi.org/10.1038/npp.2009.83.
Soraci, P., Ferrari, A., Abbiati, F. A., Del Fante, E., De Pace, R., Urso, A., & Griffiths, M. D. (2020). Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. https://doi.org/10.1007/s11469-020-00277-1.
Sousa, V. D., & Rojjanasrirat, W. (2011). Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. Journal of Evaluation in Clinical Practice, 17(2), 268–274. https://doi.org/10.1111/j.1365-2753.2010.01434.x.
Tan, B. Y. Q., Chew, N. W. S., Lee, G. K. H., Jing, M., Goh, Y., Yeo, L. L. L., Zhang, K., Chin, H.-K., Ahmad, A., Khan, F. A., Shanmugam, G. N., Chan, B. P. L., Sunny, S., Chandra, B., Ong, J. J. Y., Paliwal, P. R., Wong, L. Y. H., Sagayanathan, R., Chen, J. T., Ying Ng, A. Y., Teoh, H. L., Ho, C. S., Ho, R. C., & Sharma, V. K. (2020). Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Annals of Internal Medicine. https://doi.org/10.7326/M20-1083.
Terkawi, A. S., Tsang, S., AlKahtani, G. J., Al-Mousa, S. H., Al Musaed, S., AlZoraigi, U. S., Alasfar, E. M., Doais, K. S., Abdulrahman, A., & Altirkawi, K. A. (2017). Development and validation of Arabic version of the Hospital Anxiety and Depression Scale. Saudi Journal of Anaesthesia, 11(Suppl 1), S11–S18. https://doi.org/10.4103/sja.SJA_43_17.
Valtorta, N. K., Kanaan, M., Gilbody, S., Ronzi, S., & Hanratty, B. (2016). Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart, 102(13), 1009–1016. https://doi.org/10.1136/heartjnl-2015-308790.
Van Bavel, J. J., Baicker, K., Boggio, P. S., Capraro, V., Cichocka, A., Cikara, M., Crockett, M. J., Crum, A. J., Douglas, K. M., Druckman, J. N., Drury, J., Dube, O., Ellemers, N., Finkel, E. J., Fowler, J. H., Gelfand, M., Han, S., Haslam, S. A., Jetten, J., … Willer, R. (2020). Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour, 1–12. https://doi.org/10.1038/s41562-020-0884-z.
Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), E1729. https://doi.org/10.3390/ijerph17051729.
Witte, K. (1992). Putting the fear back into fear appeals: the extended parallel process model. Communication Monographs, 59(4), 329–349. https://doi.org/10.1080/03637759209376276.
Witte, K., & Allen, M. (2000). A meta-analysis of fear appeals: implications for effective public health campaigns. Health Education & Behavior, 27(5), 591–615. https://doi.org/10.1177/109019810002700506.
World Health Organization. (2020). Coronavirus disease (COVID-19) advice for the public. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
Xiao, H., Zhang, Y., Kong, D., Li, S., & Yang, N. (2020). Social capital and sleep quality in individuals who self-isolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 26, e923921-1–e923921-8. https://doi.org/10.12659/MSM.923921.
Zhang, S. X., Wang, Y., Rauch, A., & Wei, F. (2020). Unprecedented disruption of lives and work: health, distress and life satisfaction of working adults in China one month into the COVID-19 outbreak. Psychiatry Research, 288, 112958. https://doi.org/10.1016/j.psychres.2020.112958.
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Acknowledgments
The authors would like to acknowledge and thank Suzan Alkhodair for her help with the scale translation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration.
Informed Consent
All participants provided electronic informed consent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
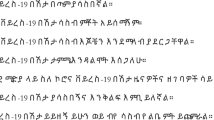
Arabic version of the Fear of COVID-19 Scale
-
1-
أنا خائف من فيروس كورونا-١٩ لأقصى حدّ
-
2-
التفكير بفيروس كورونا-١٩ يشعرني بعدم الارتياح
-
3-
أشعر بتعرق في كفيّ عندما أفكر بفيروس كورونا-١٩
-
4-
أخشى أن أفقد حياتي بسبب فيروس كورونا-١٩
-
5-
ينتابني القلق أو التوتر عندما أشاهد أخبارًا أو قصصًا عن فيروس كورونا-١٩
-
6-
لا يمكنني النوم بسبب قلقي من الإصابة بعدوى فيروس كورونا-١٩
-
7-
تتسارع دقات قلبي عندما أفكر بالإصابة بعدوى فيروس كورونا-١٩
Rights and permissions
About this article

Cite this article
Alyami, M., Henning, M., Krägeloh, C.U. et al. Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. Int J Ment Health Addiction 19, 2219–2232 (2021). https://doi.org/10.1007/s11469-020-00316-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-020-00316-x