
Abstract
A novel coronavirus disease (COVID-19) continues to challenge the whole world. The disease has claimed many fatalities as it has transcended from one country to another since it was first discovered in China in late 2019. To prevent further morbidity and mortality associated with COVID-19, most of the countries initiated a countrywide lockdown. While physical distancing and lockdowns helped in curbing the spread of this novel coronavirus, it led to massive economic losses for the nations. Positive impacts have been observed due to lockdown in terms of improved air quality of the nations. In the current research, ten tropical and subtropical countries have been analysed from multiple angles, including air pollution, assessment and valuation of health impacts and economic loss of countries during COVID-19 lockdown. Countries include Brazil, India, Iran, Kenya, Malaysia, Mexico, Pakistan, Peru, Sri Lanka, and Thailand. Validated Simplified Aerosol Retrieval Algorithm (SARA) binning model is used on data collated from moderate resolution imaging spectroradiometer (MODIS) for particulate matters with a diameter of less than 2.5 μm (PM2.5) for all the countries for the month of January to May 2019 and 2020. The concentration results of PM2.5 show that air pollution has drastically reduced in 2020 post lockdown for all countries. The highest average concentration obtained by converting aerosol optical depth (AOD) for 2020 is observed for Thailand as 121.9 μg/m3 and the lowest for Mexico as 36.27 μg/m3. As air pollution is found to decrease in the April and May months of 2020 for nearly all countries, they are compared with respective previous year values for the same duration to calculate the reduced health burden due to lockdown. The present study estimates that cumulative about 100.9 Billion US$ are saved due to reduced air pollution externalities, which are about 25% of the cumulative economic loss of 435.9 Billion US$.
Graphical abstract

Similar content being viewed by others
Introduction
Air pollution (AP) is a major problem in developing countries mainly due to rapid industrialisation and urbanization (Rai et al. 2011; Hossain and Easa 2012; Uttara et al. 2012; Mannucci and Franchini 2017). Vehicular and industrial sources seem to be a pivotal contributor to particulate pollution in urban areas (Petkova et al. 2013; Guttikunda et al. 2014; Sgrigna et al. 2015). Long-term exposure to particulate matter (PM) affects human health causing diseases such as chronic obstructive pulmonary disease (COPD), respiratory diseases, cancer and cardiovascular morbidity/mortality (Anderson et al. 2012; Kim et al. 2017; Bherwani et al. 2020a). Exposure to high PM concentrations with a diameter ≤ 2.5 μm (PM2.5) for shorter duration augment the severity of lung and heart conditions, notably affecting the quality of human life (Charron and Harrison 2005; Guarnieri and Balmes 2014). Increased PM concentration in the air may lead to poor visibility and compounded effects other than health (Nair et al. 2020).
COVID-19 outbreak was first documented in the Hubei Province’s Wuhan city, China, and it is considered as the main epicentre of SARS-CoV-2 (WHO 2020; Gautam 2020a; Gautam 2020b; Gautam and Hens 2020; Bherwani et al. 2020b; Kaur et al. 2020). Due to the outbreak of COVID-19, World Health Organization (WHO) initially declared a global public health emergency (WHO 2020; Lau et al. 2020). Now it has grown into a global pandemic and has resulted in 10 million cases just within 6 months (WHO 2020). To control the spread and related fatalities, an immediate lockdown was imposed by many countries to minimize the movement of infected people and thereby to abate the adverse health effects (Bherwani et al. 2020a, b; Wathore et al. 2020; Gautam et al. 2021). The lockdown resulted in reduced vehicular movements, staunched construction activities and halted industrial operations resulting in reduced air pollution (Bao and Zhang 2020; Bherwani et al. 2020a; Gupta et. al. 2020; Shrestha et al. 2020; Muhammad et al. 2020; Rajput et al. 2020; Ambade et al. 2021).
Despite improvements in ambient air quality as reported in several studies (Kumari and Toshniwala 2020; Venter et al. 2020; Bherwani et al. 2020a), indoor air quality showed negligible improvement (Du and Wang 2020; Ravindra et al. 2021a; Beig et al. 2021) during the period of lockdown. In rural areas, there triggered an additional requirement of fuel woods to carter the needs of extra family members who returned from their urban workplaces resulting in increased emission from cooking (Pierre et al. 2020). Ravindra et al. (2021b) reported that the transition of clean fuel cooking was hindered due to the imposed lockdown in India and households might have relapsed to traditional fuel wood cooking. Globally, there emerged a subsequent issue with biomedical waste management (BMW) due to the increased disposal rate of personal protection equipment (PPE), gloves, masks and other infectious waste beyond the installed treatment capacity (Kumar et al. 2020). To target this issue, modified guidelines were adopted in handling COVID-19-infected BMW across the globe. Bherwani et al. (2021a) in his study has highlighted the impact on Sustainable Development Goals (SDG: 1–8 & 11–17) by COVID-19 imposed lockdown. The study observed considerable improvements in terms of environmental sustainability and climate change. However, other national concerns such as employment, health, economy and social security were found to be at the highest threat.
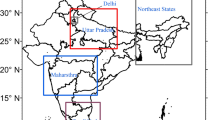
The current research discusses the air quality improvement, in terms of fine PM, for selected tropical and subtropical countries. Remote sensing-based assessment of PM2.5 concentration is conducted for 10 tropical and subtropical countries including Brazil, India, Iran, Kenya, Malaysia, Mexico, Pakistan, Peru, Sri Lanka and Thailand. A study by Mavridou et al. (2018) was used as a reference in identifying tropical and subtropical countries. Availability of data concerning satellite image, lockdown duration and national health information in addition to the Global Burden of Diseases study (GBD, 2019) was referred to ensure that selected countries covered a broader range of health risk rates (high to low) as an effect of exposure to ambient particulate matter. GBD (2019) reported mortality per 105 population for Brazil (20.11), India (70.44), Iran (49.52), Kenya (10.93) Malaysia (33.71), Mexico (29.28), Pakistan(50.88), Peru (26.2), Sri Lanka (33.23) and Thailand (45.9) attributable to ambient air particulate matter for the year 2019 (Anisah 2020; Arrieta et. al. 2014; Banjot 2019; Viscusi and Masterman 2017; Walker et. al. 2018; Yong and Shafie 2016; Subramanian et. al. 2018; Thanaviratananich et. al. 2016). Further assessment in terms of reduction in health impacts is assessed in monetary terms. The novelty of the work is that it uses satellite data to assess the change in concentration of PM2.5 for the tropical and subtropical countries from the year 2019 to 2020 during the COVID-19 lockdown period and assesses the health benefits of reduced air pollution in monetary terms. Such holistic studies are seldom done which give a detailed analysis of air pollution reduction at the country level along with air pollution health burden. Figure 1 shows the geographical locations of all the countries included in the study. To add to the originality, the air pollution externalities (APE) reduction during the COVID-19 lockdown is compared with the economic damage suffered by each country to highlight the environmental benefits of the lockdown. Selecting countries limited to higher health risk rates (or high PM2.5 concentration) may only result in environmental benefit as a result of lockdown. To eliminate such biasness in the current study, larger window of health risk rates was adopted while finalizing the countries.

Geographical locations of the study area
Methodology
Population (N)
The population of the above-mentioned countries in the years 2019 and 2020 is collected for evaluation of health damages subjected to mortality/morbidity due to air pollution in a particular country. The population has increased in millions from 2019 to 2020 by 1.6 (211 to 212.6) in Brazil, 14 (1366 to 1380) in India, 1.3 (82.9 to 83.9) in Iran, 1.2 (52.6 to 53.8) in Kenya, 1.0 (31.9 to 32.9) in Malaysia, 1.3 (127.6 to 128.9) in Mexico, 4.3 (216.6 to 220.9) in Pakistan, 0.4 (32.5 to 32.9) in Peru, 0.1 (21.3 to 21.4) in Sri Lanka and 0.2 (69.6 to 69.8) in Thailand (Worldometer 2019, 2020).
Air quality
Satellite data has been prominent among the researchers in carrying out the environment and climate change related studies due to its advanced spatial and temporal coverage (Bherwani et al. 2020c). Moderate resolution imaging spectroradiometer (MODIS) data is used for determining the PM2.5 concentration of each country for January, February, March, April and May 2019 and 2020. The acquisition details are given in Table 1.
Several studies using complex chemical transport model (CTM) (Liu 2004; Van Donkelaar et al. 2012; Krishna et al. 2019; Srivastava 2020), machine learning regression models (Xu and Zhang 2020; Ma et al. 2014; Lai et al. 2014; Gupta and Christopher 2008) and combination of both (Van Donkelaar et al. 2016) exist which configure a relation between AOD and PM2.5. Since there exists no such model as the best model, we relied on model simplicity and performance accuracy in selecting the most suitable model for the current study. CTM was eliminated as it requires larger time, energy and resources in collecting relevant data corresponding to PM2.5 (Van Donkelaar et al. 2010). Chu et al. (2016) in his study mentioned that PM2.5 prediction improves while incorporating meteorological parameters with AOD when compared to simple linear AOD to PM2.5model. To retrieve the PM2.5 from aerosol optical depth (AOD) by MODIS (MOD08_M3), a newly developed algorithm is used in ArcGIS. This advanced method comprises of validated Simplified Aerosol Retrieval Algorithm (SARA) and retrieves PM2.5 concentration from AOD data through binning of meteorological variables (Bilal et al. 2013, 2017). This model is based on meteorological variables which can be used to achieve a higher correlation between AOD and PM2.5.
The details of the retrieval mechanism is given in Fig. 2.

Retrieval of PM2.5 from MODIS AOD data
Exposure assessment
Health effects such as respiratory effects, chronic obstructive pulmonary diseases, cardiovascular diseases and mortality attributable to ambient air pollution specific to PM2.5 during the period of lockdown in 2020 and for the same period in 2019 were estimated using the linear exposure-response curve method. This method was assessed by considering relative risk due to the mean concentration of PM2.5 pollutant, baseline incidence cases per 105 population, pollution attributable to risk (PAR) corresponding to mortality and morbidity health effects and the total population in 2019 and 2020 for the countries (N). Eqs. (1)–(4) were used for estimating the mortality and morbidity cases for the study period and countries (Bherwani et al. 2020a).
where Rrc is the relative risk for exposed concentration, Cmis the monitored ambient mean air quality concentration of pollutant PM2.5. Cpis the ambient air quality standards from WHO guidelines for PM2.5 pollutant. Rr and Ieare the relative risk and baseline incidence for the pollutant PM2.5 and are shown in Table 2. ρ(c) proportion of pollution exposure to the pollutant (100% is being exposed to the pollutant concentration is considered in our study). Ine is the number of people affected due to air pollution.
Valuation of air pollution externalities
Improved health effects assed in monetary terms can raise awareness among policy and decision makers regarding the need in identifying strategies to curb growing air pollution in the countries (Bherwani et al. 2020d). To calculate the monetary burden of health risk for morbidity and mortality, cost of illness (COI), disability-adjusted life years (DALY) and value of statistical life (VSL) methods are used. COI and DALY are used for monetising morbidity endpoint, and the VSL method was used for mortality endpoint for all above-mentioned countries (Bherwani 2020a, b). VSL of each country assessment was done based on the insurance settlements and the values are given as Supplementary Table-1. These VSL values are inflated to 2019 (The World Bank 2019). Eq. (5) shows the calculation of monetary damages due to mortality following (Bherwani et al. 2020a).
Morbidity is monetised by using the COI and DALY and the sum of both methods were carried out to assess total morbidity damage value. Morbidity by COI method included treatment cost of each disease in the country. It includes hospital admission, medical cost, travelling cost and lost day. COI of each disease in each country is given in Supplementary Table-2 and are converted to US$ and inflated to 2019 for uniformity. The benefit transfer method was used to estimate COI value for countries such as Sri Lanka, Brazil and Pakistan employing exchange rate (ER) and inflation rate (IR) on existing illness cost value for a country using Eq. (6) (Bherwani et al. 2020a).
DALY method was used to estimate the years of life opportunity lost due to morbidity and mortality. DALY data of each country was taken from the WHO database (WHO 2016). The details are highlighted in Supplementary Table-3. DALY method for morbidity indicates the number of years of life lost for an individual due to illness. It can be calculated using the annual per capita income of each individual. Per capita income (PCI) of each country was taken from the referenced literature and inflated in 2019 as shown in the Supplementary Table-4 (The World bank 2019; Observer Research Foundation (ORF) 2020; Statista 2020). Eq. (7) is used to calculate the morbidity damage estimation by DALY method (Bherwani et al. 2020a).
Based on Eqs. (1)–(7), mortality and morbidity attributable to air pollution were evaluated. It was observed that countries have suffered huge losses due to COVID-19 which was reflected in the reduced gross domestic product (GDP). This loss was compared with the reduced health burden of the countries. The losses in GDP was calculated using the International Monetary Fund (IMF 2020) GDP percentage change values and assuming that the growth rate would have remained the same for 2020 as well, except for Iran where the last positive change was referred to as the base value. The GDP erosion was reported in 2019 values considering average inflation of 3.56%.
Results and discussion
Air quality
In many countries, the lockdown was imposed due to the outbreak of unrestrained growth of COVID-19. In this study, SARA-derived MODIS data was used for PM2.5 concentration determination using the methodologies as explained above. The MODIS data obtained is shown as averaged maps for 2019 and 2020 in Fig. 3 for each of the ten countries.




MODIS obtained images for tropical and subtropical countries considered in the study for the months of January–May 2019 and 2020
For all 10 countries, the PM2.5 data from January to May for the years 2019 and 2020 is retrieved from MODIS using SARA binning model and is presented (Fig. 3). From the figure, it can be observed that the pollution increased in 2020 in some countries while decreased in others as compared to 2019. The monthly variation in PM2.5 (January–May) obtained from MODIS for each of the countries for the years 2019 and 2020 was shown in Fig. 4. Overall, it was clear from Fig. 4 that the concentration of PM2.5 dropped after the lockdown in 2020 sooner or later. The detailed monthly PM2.5 average was shown in Supplementary Table-5.

a Variation in monthly mean, maximum and minimum PM2.5 concentration for the years 2019 and 2020 (Jan–May) in the countries; b Monthly difference in PM2.5 concentration for the countries between 2020 and 2019 (2020 minus 2019)
It is evident from the figure, since the starting of lockdown, in March 2020 for most of the countries, the PM2.5 levels dropped resulting in lower health burden and corresponding externalities. Lockdown across the globe has strictly restricted various anthropogenic activities which were the primary sources of pollution and hence would have improved the air quality. The mean values are averaged for the months in which the PM2.5 concentration of 2020 has fallen below the mean value in 2020. The averaged values thus generated are shown in Table 3. An overall reduction of the range 5.0–34% in PM2.5 concentration was observed in the study areas during the lockdown when compared to the same period last year. The highest reduction was observed for Sri Lanka (34.1%). followed by Mexico (27.3%), India (16.4%), Malaysia (15.4%), Iran (14.3%), Pakistan (13.6%), Brazil (12.0%), Kenya (10.2%), Thailand (5.2%) and Peru (5.0%). Satellite-based global studies were limited for comparison. Comparison with previous studies can result in a mismatch as the studies were limited to specific cities in the country using ground-based air quality stations and for various timescale (lockdown and pre-lockdown) durations.
Studies reported that there existed a fair reduction in PM2.5 during lockdown compared to pre-lockdown situation. Colombo, in Sri Lanka, showed 8% improvement in overall air quality compared to the previous years (Kandari and Kumar 2021). Kutralam-Muniasamy et al. (2020) reported that Mexico exhibited a reduction of 19% during lockdown months (April and May 2020) when compared to the historic trend (2015–2019). These values reported in the previous studies mismatch with the current study as we have analysed using the satellite data having robust spatial coverage as compared to ambient air quality monitoring stations. For India, Venter et al. (2020) reported a reduction of 15 μg/m3 for the year 2020 (Jan–May) compared to the previous 3 years for the same period. Sharma et al. (2020) reported a reduction up to 43% in PM2.5 as recorded by the Continuous Ambient Air Quality Monitoring Stations (CAAQMS) across various cities in India during the days of stringent lockdown (16 March to 14 April 2020). Singh et al. (2020) reported an improvement up to 60% as the lockdown extended until May 3, 2020. The increase observed during March 2020 as shown in Fig. 4 was well captured in the study conducted by Kumar et al. (2020) reporting an increase of 20–100% in aerosol loading at northern regions of India. For Brazil, Pakistan, Malaysia, Iran and Peru, there existed very limited studies on PM2.5 levels during lockdown. Tello-Leal et al. (2020) reported a reduction of 44.52% for Victoria City, Brazil, during lockdown compared to the pre-lockdown period. For Thailand, no larger difference in PM2.5 concentration was observed due to the wildfire episode causing smoke loading (Venter et al. 2020). However, just considering the lockdown period (March–May 2020), 26–55% reduction in PM2.5 was reported by Kaewrat and Janta (2021) compared to pre-lockdown.
Valuation of air pollution health impacts
Emissions of pollutants beyond the threshold limits result in adverse impacts on human health and other natural environments (Bherwani et al. 2020a, b). In the current study, we are focusing mainly on human health damages attributable to PM2.5. Air quality guidelines of 10 μg/m3 as recommended by World Health Organization (WHO) for PM2.5 pollutant as the lower end of the range of concentration over which adverse health effects were observed (https://datacatalog.worldbank.org/pm25-pollution-population-exposed-levels-exceeding-who-interim-target-1-value-total-1) and was taken as reference concentration for health risk assessment. From Table 3, PM2.5 concentration was found beyond the minimum threshold limits of 10 μg/m3 in 2019 and 2020. By using this PM2.5 data, the total number of cases subjected to mortality and morbidity was calculated using Eqs. (1)–(4). Morbidity and mortality parameters are considered in the study is detailed in Table 2.
Table 4 shows the morbidity and mortality attributable to air pollution aggregated for April and May of 2019 and 2020. Total morbidity (respiratory diseases, cardiovascular diseases and COPD) cases showed a reduction of the range 4.7–38.4% over the study areas. Total mortality cases reduction was observed to be of range 5.2–40%. The highest and lowest reduction in morbidity and mortality cases was observed for Sri Lanka and Thailand respectively. Country-wise, VSL for mortality and COI for each disease were taken from the data collated in Supplementary Table 2 (Aljunid et al. 2013; Alvis-Guzmán et al. 2015). The damages were assessed using Eq. (6). Further, the damages are not restricted to treatment costs, but the disability of a person results in inability to work which is valued using DALY. This inability of working is reflected in income loss which can be valued using per capita income as given in Supplementary Table 4 and solved using Eq. (7).
The economic burden due to mortality and morbidity attributable to air pollution is assessed. Tables 5 and 6 shows the damages in terms of Million US$ due to morbidity and mortality respectively. Average economic loss in morbidity was estimated to be 638.7 Million US$ for the year 2020 and was 21.3% lower than the previous year. For the year 2020, Mexico showed the highest economic loss due to morbidity at 2725. 8 Million US$ followed by India at 1546.6 Million US$. The lowest being recorded at 5.18 Million US$ for Sri Lanka. The overall morbidity damage cost assessed is not just dependent on PM2.5 concentration and population but also on country specific DALY values as detailed in Supplementary Table-3. Hence, it is obvious that despite having a lower morbidity case recorded at Mexico than India (as in Table 4), higher DALY value for the country has resulted in larger economic loss. Mortality damage was assessed by total mortality cases which is cumulative of respiratory and cardiovascular disease mortality. Average economic loss estimated for the study areas due to total mortality in the year 2020 was 46.89 Billion US$ and was 17.4% lower than the previous year. For 2020, India showed highest damage of 195.7 Billion U$ and lowest being Kenya at 2.2 Billion U$. Despite, Thailand being at higher end of Pollution level than India, total economic loss due mortality was lower than India due to larger difference (14.1 Million) in population.
Economic loss due to lockdown in the above-mentioned countries due to outbreak of COVID-19 is shown in Table 7.
Table 7 indicates that each of the countries analysed recovered some of the value of GDP lost due to the reduced health burden of PM2.5. The recovery in terms of loss of GDP varies between as low as 3% for Peru to as high as 79% for Sri Lanka. The average recovery is about 25% which is enormous given that the reduced footprint of humans is also saving them from deadly COVID-19. The overall improvement in air quality and associated APE also depends on lockdown strategies within the countries having widely distributed urban agglomeration and degree of implementation by the concerned local governments. The varying meteorological factors and natural source contributions across topographies have a substantial role in influencing the ambient air quality (Bherwani et al. 2021b). Since these factors are subjective, there exists huge scope of investigating their impacts during lockdown scenarios across the globe.
Conclusion
The novel coronavirus has spread almost in all countries and has taken many casualties through this deadly disease COVID-19, as it has spread from continent to continent. The reproduction number of SARS-CoV-2 is also very high, and hence it penetrates among the population very fast. The first line of defence against such troublesome pandemics has always been physical hygiene. For this virus, physical distancing has been one of the most effective ways to control its spread. Most countries implemented countrywide lockdown strategies to strictly implement physical distancing as soon as the cases started rising. Similar is the case of countries including Brazil, India, Iran, Kenya, Malaysia, Mexico, Pakistan, Peru, Sri Lanka and Thailand. The lockdowns in these countries were implemented in March 2020.
With COVID-19 lockdowns, the state of the environment seemed to improve due to reduced anthropogenic activities. Similar is the case with air pollution. AOD is retrieved from MODIS for ten countries from January to May for the years 2019 and 2020 to analyse the data in detail concerning air pollution. The AOD data is converted into PM2.5 concentration using SARA binning model. On an average, after the lockdown, the difference between PM2.5 concentration from 2019 to 2020 started dropping for all countries, from 53.3 μg/m3 in March to 6.9 μg/m3 in April to −9.8 μg/m3 in May (negative sign indicates lower concentration in 2020 as compared to 2019). This suggests that anthropogenic activities are mainly responsible for air pollution in these countries, and with its reduction, the air pollution was drastically reduced.
Another critical aspect explored is linked with the reduced health burden of air pollution due to this lockdown. The baseline incidence and relative risk values are used for various morbidity and mortality-related aspects of air pollution. Respiratory disorder, cardiovascular diseases and COPD are evaluated for these countries. Furthermore, the valuation of this reduced health burden is carried out using econometric methods including COI, VSL and PCI. Figure 5 shows the reduced APE.

Reduced health burden vis-à-vis economic loss
The biggest loss in terms of absolute numbers of GDP appears to be for Brazil with a loss of 140.95 Bn US$ followed by Mexico and India with a loss of 80.23 Bn US$ and 65.38 Bn US$ due to lockdown respectively (France 24 2020; Financial Express 2020; Financial Tribune 2020). While the health burden reduction is highest for India in terms of absolute numbers i.e. 38.6 Bn US$ followed by Mexico and Brazil. However, percentage recovery due to reduced health burden is highest for Sri Lanka with 79% while India is second highest with 59%.
Given the above conclusions, following aspects need urgent attention and form the scope of future research:
-
1.
Lockdown and losses: It is true that lockdown had created enormous losses and has impacted GDP of the countries; however, there are benefits in terms of improvement of the environment, which is demonstrated in terms of AP reduction in this paper. Similarly, exploration should be done for other environmental factors such as water pollution, solid waste generation, climate change etc.
-
2.
Country’s response and local meteorology: Although the lockdowns were initiated in similar timeframes, the response of each country was different as evident by the time taken by each country to show a reduction in air pollution. This indicates that countries local conditions play a significant role when it comes to assimilating the pollution. Some of the factors which should be researched in detail including, but not limited to, are meteorology, sources of pollution, land use etc. to actually understand and forecast, as the need be.
-
3.
Air pollution and health damage: It is clear that air pollution is associated with substantial health burden and the paper clearly demonstrates that a slight reduction in air pollution can lead to enormous savings. This creates a doorway for policymakers to put forth the agenda of environmental prevention and restoration on a concrete foot with evidence of monetary benefits.
-
4.
Background concentration: The pandemic and lockdown have presented a distinctive opening for researches to understand the baseline and background concentration of pollutants in their respective countries and the world overall. While the current paper restricts itself to air pollution-related analysis, the research can be extended to other types of pollution as well as discussed above.
-
5.
Possible next steps: The proposed future directions in terms of background concentration studies, economic evaluation of impacts and the study of local parameters can be used in overall holistic researches such as environmental impact assessments and carrying capacity analysis. These areas will also contribute to policy and decision making when developmental scenarios are weighed against environmental conservation and restoration.
Conclusively, it can be inferred that that air pollution increase is mostly because of anthropogenic activities, and it leads to economic losses due to associated health damages. In summary, the current research demonstrates that there is a bright side of the lockdown in terms of an improved environment. The current study focuses on specific countries, which are less explored in terms of conjugate effects of COVID-19; going forward, the approach can be applied to other countries as well. Further, the research concludes that there is a lot to explore on similar lines and that this pandemic although has created devastation but has also presented a unique opportunity to study the environment in detail and from a different lens.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
References
Aljunid S, Namaitjiang M, Al-Abed A, Amrizal M, Zafar A, De Rosas-Valera M, Encluna J, Rosminah M, Azmi S (2013) The burden of pneumonia in Malaysia, Indonesia and Philippines. Value Health 16(7):A369
Alvis-Guzmán N, Marin-Correa C, Castañeda-Orjuela C, Sanchez-Ruiz C, Carrasquilla-Sotomayor M, Sanchez F, Mena R, Mejía H (2015) Hospitalization costs due to severe acute respiratory infection (SARI) in three central American countries. Value Health 18(3):A253
Ambade B, Sankar TK, Kumar, A., Gautam, A.S., Gautam, S. (2021). COVID-19 lockdowns reduce the Black carbon and polycyclic aromatic hydrocarbons of the Asian atmosphere: source apportionment and health hazard evaluation. Environmental Development and Sustainability (https://doi.org/10.1007/s10668-020-01167-1)
Anderson JO, Thundiyil JG, Stolbach A (2012) Clearing the air: a review of the effects of particulate matter air pollution on human health. Journal of Medical Toxicology 8(2):166–175
Anisah S (2020) Malaysia sees 2.4 billion ringgit a day of losses from lockdown. https://www.bloomberg.com/news/articles/2020-04-25/malaysia-sees-2-4-billion-ringgit-a-day-of-losses-from-lockdown Accessed April 25, 2020
Arrieta O, Quintana-Carrillo RH, Ahumada-Curiel G, Corona-Cruz JF, Correa-Acevedo E, Zinser-Sierra J, De La Mata-Moya D, Mohar-Betancourt A, Morales-Oyarvide V, Reynales-Shigematsu LM (2014) Medical care costs incurred by patients with smoking-related non-small cell lung cancer treated at the National Cancer Institute of Mexico. Tob Induc Dis 12(1):25
Banjot K (2019) Indians are getting sick mostly due to infections: NSSO report. https://www.downtoearth.org.in/news/health/indians-are-getting-sick-mostly-due-to-infections-nsso-report-67913 Accessed April 25, 2020
Bao R, Zhang A (2020). Does lockdown reduce air pollution? Evidence from 44 cities in northern China. Science of the Total Environment, 139052
Beig G, Korhale N, Rathod A, Maji S, Sahu SK, Dole S, Latha R, Murthy BS (2021) On modelling growing menace of household emissions under COVID-19 in Indian metros. Environ Pollut 272:115993
Bherwani H, Nair M, Musugu K, Gautam S, Gupta A, Kapley A, Kumar R (2020a) Valuation of air pollution externalities: comparative assessment of economic damage and emission reduction under COVID-19 lockdown. Air QualAtmos Health 13:683–694. https://doi.org/10.1007/s11869-020-00845-3
Bherwani H, Anjum S, Kumar S, Gautam S, Gupta A, Kumbhare H, Anshul A, Kumar R (2020b) Understanding COVID-19 transmission through Bayesian probabilistic modelling and GIS based Voronoi approach: a policy perspective. Environ Dev Sustain. https://doi.org/10.1007/s10668-020-00849-0
Bherwani H, Singh A, Kumar R (2020c) Assessment methods of urban microclimate and its parameters: a critical review to take the research from lab to land. Urban Clim 34:100690
Bherwani H, Nair M, Kapley A, Kumar R (2020d) Valuation of ecosystem services and environmental damages: an imperative tool for decision making and sustainability. Eur J Sustain Dev Res 4(4):em0133. https://doi.org/10.29333/ejosdr/8321
Bherwani H, Gautam S, Gupta A (2021a) Qualitative and quantitative analyses of impact of COVID-19 on sustainable development goals (SDGs) in Indian subcontinent with a focus on air quality. Int J Environ Sci Technol 18:1019–1028
Bherwani H, Anjum S, Gupta A, Singh A, Kumar R (2021b) Establishing influence of morphological aspects on microclimatic conditions through GIS-assisted mathematical modeling and field observations. Environ Dev Sustain
Bilal M, Nichol JE, Bleiweiss MP, Dubois D (2013) A simplified high resolution MODIS aerosol retrieval algorithm (SARA) for use over mixed surfaces. Remote Sens Environ 136:135–145
Bilal M, Nichol JE, Spak SN (2017) A new approach for estimation of fine particulate concentrations using satellite aerosol optical depth and binning of meteorological variables. Aerosol Air Qual Res 17:356–367
Brouwer ED, Watkins D, Olson Z, Goett J, Nugent R, Levin C (2015) Provider costs for prevention and treatment of cardiovascular and related conditions in low-and middle-income countries: a systematic review. BMC Public Health 15(1):1183
Charron A, Harrison RM (2005) Fine (PM2. 5) and coarse (PM2. 5-10) particulate matter on a heavily trafficked London highway: sources and processes. Environ Sci Technol 39(20):7768–7776
Chu Y, Liu Y, Li X, Liu Z, Lu H, Lu Y, Mao Z, Chen X, Li N, Ren M, Liu F, Tian L, Zhu Z, Xiang H (2016) A review on predicting ground PM2.5 concentration using satellite aerosol optical depth. Atmosphere 7(10):129. https://doi.org/10.3390/atmos7100129
Du W, Wang G (2020) Indoor air pollution was nonnegligible during COVID-19 lockdown. Aerosol Air Qual Res 20:1851–1855
Farahani AV, Salamzadeh J, Rasekh HR, Najafi S, Mosadegh V (2018) The availability and affordability of cardiovascular medicines for secondary prevention in Tehran province (Iran). Iranian Journal of Pharmaceutical Research: IJPR 17(Suppl):64
Figueroa-Lara A, Gonzalez-Block MA, Alarcon-Irigoyen J (2016) Medical expenditure for chronic diseases in Mexico: the case of selected diagnoses treated by the largest care providers. PLoS One 11(1):e0145177
Financial Express (2020). Pakistan says COVID-19 to take heavy toll on economy, fears 18.5 million job losses. https://www.financialexpress.com/economy/pakistan-says-COVID-19-to-take-heavy-toll-on-economy-fears-18-5-million-job-losses/1918169/ Accessed April 03, 2020
Financial Tribune (2020). COVID-19 to adversely impact 15 percent of Iranian GDP. https://financialtribune.com/articles/domestic-economy/102761/COVID-19-to-adversely-impact-15-percent-of-iranian-gdp Accessed April 10, 2020
Foo J, Landis SH, Maskell J, Oh YM, van der Molen T, Han MK, Mannino DM, Ichinose M, Punekar Y (2016) Continuing to confront COPD international patient survey: economic impact of COPD in 12 countries. PLoS One 11(4)
France 24 (2020). Brazil faces economic collapse in 30 days, minister says. https://www.france24.com/en/20200508-brazil-economy-minister-paulo-guedes-jair-bolsonaro-COVID-19-coronavirus-lockdown-protests Accessed 08 May 2020
Gautam S (2020a) The influence of COVID – 19 on air quality in India: a boon or inutile. Bull Environ Contam Toxicol 104(6):724–726
Gautam S (2020b). COVID – 19: Air pollution remains low as people stay at home. Air Quality Atmosphere and Health
Gautam S, Hens L (2020). COVID-19: impact by and on the environment, health and economy. Environ Dev Sustain
Gautam AS, Kumar S, Gautam S, Anand A, Joshi A, Bauddh K, Singh K (2021). Pandemic induced lockdown as a boon to the Environment: trends in air pollution concentration across India. Asia-Pacific Journal of Atmospheric Sciences. https://doi.org/10.1007/s13143-021-00232-7
Gheorghe A, Griffiths U, Murphy A, Legido-Quigley H, Lamptey P, Perel P (2018) The economic burden of cardiovascular disease and hypertension in low-and middle-income countries: a systematic review. BMC Public Health 18(1):975
Ghoshal AG, Ravindran GD, Gangwal P, Rajadhyaksha G, Cho SH, Muttalif ARBA, Lin HC, Thanaviratananich S, Bagga S, Faruqi R, Sajjan S (2016) The burden of segregated respiratory diseases in India and the quality of care in these patients: results from the Asia-Pacific burden of respiratory diseases study. Lung India: official organ of Indian Chest Society 33(6):611
Guarnieri M, Balmes JR (2014) Outdoor air pollution and asthma. Lancet 383(9928):1581–1592
Gupta P, Christopher SA (2008) Seven year particulate matter air quality assessment from surface and satellite measurements. Atmos Chem Phys 8:3311–3324
Gupta A, Bherwani H, Gautam S, Anjum S, Musugu K, Kumar N, Anshul A, Kumar R (2020) Air pollution aggravating COVID-19 lethality? Exploration in Asian cities using statistical models. Environ Dev Sustain. https://doi.org/10.1007/s10668-020-00878-9
Guttikunda SK, Goel R, Pant P (2014) Nature of air pollution, emission sources, and management in the Indian cities. Atmos Environ 95:501–510
Hossain KM, Easa SM (2012) Pollutant dispersion characteristics in Dhaka city, Bangladesh. Asia-Pac J Atmos Sci 48(1):35–41
IMF. (2020). Real GDP growth. https://www.imf.org/external/datamapper/NGDP_RPCH@WEO/THA?year=2020 Accessed April 2020
Kaewrat J, Janta R (2021) Effect of COVID-19 prevention measures on air quality in Thailand. Aerosol Air Qual Res 21:200344
Kandari R, Kumar A (2021) COVID-19 pandemic lockdown: effects on the air quality of South Asia. Environmental Sustainability
Kaur S, Bherwani H, Gulia S, Vijay R, Kumar R (2020) Understanding COVID-19 transmission, health impacts and mitigation: timely social distancing is the key. Environ Dev Sustain
Kermani M, Goudarzi G, Shahsavani A, Dowlati M, Asl FB, Karimzadeh S, Jokandan SF, Aghaei M, Kakavandi B, Rastegarimehr B, Ghorbani-Kalkhajeh S (2018) Estimation of short-term mortality and morbidity attributed to fine particulate matter in the ambient air of eight Iranian cities. Annals of Global Health 84(3):408
Kim HJ, Choi MG, Park MK, Seo YR (2017) Predictive and prognostic biomarkers of respiratory diseases due to particulate matter exposure. Journal of Cancer Prevention 22(1):6
Koul PA, Nowshehr AA, Khan UH, Jan RA, Shah SU (2019) Cost of severe chronic obstructive pulmonary disease exacerbations in a high burden region in North India. Annals of Global Health 85(1)
Krishna RK, Ghude SD, Kumar R, Beig G, Kulkarni R, Nivdange S, Chate D (2019) Surface PM2.5 estimate using satellite-derived aerosol optical depth over India. Aerosol Air Qual Res 19:25–37
Kumar H, Azad A, Gupta A, Sharma J, Bherwani H., Labhsetwar NK, Kumar R (2020). COVID-19 Creating another problem? Sustainable solution for PPE disposal through LCA approach. Environ Dev Sustain
Kumari P, Toshniwala D (2020) Impact of lockdown on air quality over major cities across the globe during COVID-19 pandemic. Urban Clim 34:100719
Kutralam-Muniasamy, G., Pérez-Guevara, F., Roy, P.D., Elizalde-Martínez, I., & Shruti, V.C (2020). Impacts of the COVID-19 lockdown on air quality and its association with human mortality trends in megapolis Mexico City. Air QualAtmos Health
Lai HK, Tsang H, Thach TQ, Wong CM (2014) Health impact assessment of exposure to fine particulate matter based on satellite and meteorological information. Environ Sci Process Impacts 16:239–246
Lau H, Khosrawipour V, Kocbach P, Mikolajczyk A, Schubert J, Bania J, Khosrawipour T (2020) The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J Travel Med 27(3):taaa037
Liu Y (2004). Mapping annual mean ground-level PM2.5 concentrations using multiangle imaging spectroradiometer aerosol optical thickness over the contiguous United States. J Geophys Res 109
Ma Z, Hu X, Huang L, Bi J, Liu Y (2014) Estimating ground-level PM2.5 in China using satellite remote sensing. Environ Sci Technol 48:7436–7444
Maji KJ, Dikshit AK, Deshpande A (2017) Human health risk as a basis for prioritizing air quality monitoring stations in a megacity: a case study. Arab J Geosci 10(18):394
Maji KJ, Ye WF, Arora M, Nagendra SS (2018) PM2.5-related health and economic loss assessment for 338 Chinese cities. Environ Int 121:392–403
Mannucci PM, Franchini M (2017) Health effects of ambient air pollution in developing countries. Int J Environ Res Public Health 14(9):1048
Mavridou A, Pappa O, Papatzitze O, Dioli C, Kefala AM, Drossos P, Beloukas A (2018) Exotic tourist destinations and transmission of infections by swimming pools and hot springs—a literature review. Int J Environ Res Public Health 15:2730
Miri M, Derakhshan Z, Allahabadi A, Ahmadi E, Conti GO, Ferrante M, Aval HE (2016) Mortality and morbidity due to exposure to outdoor air pollution in Mashhad metropolis, Iran. The AirQ model approach. Environ Res 151:451–457
Muhammad S, Long X, Salman M (2020). COVID-19 pandemic and environmental pollution: a blessing in disguise?. Science of The Total Environment, 138820
Nair MM, Bherwani H, Kumar S, Gulia S, Goyal SK, Kumar R (2020). Assessment of contribution of agricultural residue burning on air quality of Delhi using remote sensing and modelling tools. Atmospheric Environment, 117504
Observer Research Foundation (ORF) (2020). The economic cost of COVID-19 is bigger than the great depression. https://www.orfonline.org/expert-speak/the-economic-cost-of-COVID-19-is-bigger-than-the-great-depression-65730/ Accessed May 06, 2020
Petkova EP, Jack DW, Volavka-Close NH, Kinney PL (2013) Particulate matter pollution in African cities. Air Quality, Atmosphere & Health 6(3):603–614
Pierre S, Alessandra D, Evgenios A, Feng Z, Xu X, Elena P, Jose J, Vicent C (2020) Amplified ozone pollution in cities during the COVID-19 lockdown. Sci Total Environ 735:139542
Rai R, Rajput M, Agrawal M, Agrawal SB (2011) Gaseous air pollutants: a review on current and future trends of emissions and impact on agriculture. J Sci Res 55(771):1
Rajput H, Changotra R, Rajput P, Gautam S, Gollakota ARK, Arora AS (2020). A shock like no other: coronavirus rattles commodity markets. Environmental Development and Sustainability
Ravindra K, Singh T, Biswal A, Singh V, Mor S (2021a). Impact of COVID-19 lockdown on ambient air quality in megacities of India and implication for air pollution control strategies. Environ Sci Pollut Res
Ravindra K, Kaur-Sidhu M, Mor S, Chakma J, Pillarisetti A (2021b) Impact of the COVID-19 pandemic on clean fuel programmes in India and ensuring sustainability for household energy needs. Environ Int 147:106335
Rezvanfar MA, Kebriaeezadeh A, Moein M, Nikfar S, Gharibnaseri Z, Abdollahi-Asl A (2013) Cost analysis of childhood asthma in Iran: a cost evaluation based on referral center data for asthma and allergies. Journal of Research in Pharmacy Practice 2(4):162
Sgrigna G, Sæbø A, Gawronski S, Popek R, Calfapietra C (2015) Particulate matter deposition on Quercus ilex leaves in an industrial city of Central Italy. Environ Pollut 197:187–194
Sharma S, Zhang M, Anshika, Gao J, Zhang H, Kota SH (2020) Effect of restricted emissions during COVID-19 on air quality in India. Science of Total Environment 728:138878
Shrestha, A.M., Shrestha, U.B., Sharma, R., Bhattarai, S., Tran, H.N.T., & Rupakheti, M. (2020). Lockdown caused by COVID-19 pandemic reduces air pollution in cities worldwide
Singh V, Singh S, Biswal A, Kesarkar AP, Mor S, Khaiwal R (2020) Diurnal and temporal changes in air pollution during COVID-19 strict lockdown over different regions of India. Environ Pollut 266(3):115368
Srivastava N (2020) Association of modeled PM2.5 with aerosol optical depth: model versus satellite. Nat Hazards 102:689–705
Statista (2020). Estimated cost of the coronavirus (COVID-19) lockdown on the Indian economy in 2020. https://www.statista.com/statistics/1111599/india-estimated-economic-cost-of-coronavirus-lockdown/ Accessed April 14, 2020
Subramanian S, Gakunga R, Kibachio J, Gathecha G, Edwards P, Ogola E, Yonga G, Busakhala N, Munyoro E, Chakaya J, Ngugi N (2018) Cost and affordability of non-communicable disease screening, diagnosis and treatment in Kenya: patient payments in the private and public sectors. PLoS One 13(1):e0190113
Tello-Leal E, Barbara A, Macías-Hernández (2020). Association of environmental and meteorological factors on the spread of COVID-19 in Victoria, Mexico, and air quality during the lockdown, Environmental Research 110442
Thanaviratananich S, Cho SH, Ghoshal AG, Muttalif ARBA, Lin HC, Pothirat C, Chuaychoo B, Aeumjaturapat S, Bagga S, Faruqi R, Sajjan S (2016) Burden of respiratory disease in Thailand: results from the APBORD observational study. Medicine 95(28):e4090
The World bank. (2019), Inflation, GDP deflator (annual %/), https://data.worldbank.org/indicator/NY.GDP.DEFL.KD.ZG. Accessed April 2020
Torabipour A, Hakim A, Angali KA, Dolatshah M, Yusofzadeh M (2016) Cost analysis of hospitalized patients with chronic obstructive pulmonary disease: a state-level cross-sectional study. Tanaffos 15(2):75
Uttara S, Bhuvandas N, Aggarwal V (2012) Impacts of urbanization on environment. International Journal of Research in Engineering and Applied Sciences 2(2):1637–1645
Van Donkelaar A, Martin RV, Brauer M, Kahn R, Levy R, Verduzco C, Villeneuve PJ (2010) Global estimates of ambient fine particulate matter concentrations from satellite-based aerosol optical depth: development and application. Environ Health Perspect 118:847–855
Van Donkelaar A, Martin RV, Pasch AN, Szykman JJ, Zhang L, Wang YX, Chen D (2012) Improving the accuracy of daily satellite-derived ground-level fine aerosol concentration estimates for North America. Environ Sci Technol 46:11971–11978
Van Donkelaar A, Martin RV, Brauer M, Hsu NC, Kahn RA, Levy RC, Lyapustin A, Sayer AM, Winker DM (2016) Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ Sci Technol 50:3762–3772
Venter ZS, Aunan K, Chowdhury S, Lelieveld J (2020) COVID-19 lockdowns cause global air pollution declines. Proc Natl Acad Sci 117(32):18984–18990
Viscusi WK, Masterman CJ (2017) Income elasticities and global values of a statistical life. Journal of Benefit-Cost Analysis 8(2):226–250
Walker IF, Garbe F, Wright J, Newell I, Athiraman N, Khan N, Elsey H (2018) The economic costs of cardiovascular disease, diabetes mellitus, and associated complications in South Asia: a systematic review. Value in health regional issues 15:12–26
Wathore R, Gupta A, Bherwani H, Labhasetwar N (2020) Understanding air and water borne transmission and survival of coronavirus: insights and way forward for SARS-CoV-2. Sci Total Environ 749:141486. https://doi.org/10.1016/j.scitotenv.2020.141486
World Health Organization. (2016). Health Statistics and Informative Systems. https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html. Accessed April 2020
World Health Organization. (2020). There is a outbreak of Corona Virus (COVID-19) disease. https://www.who.int/health-topics/coronavirus#tab=tab_1. Accessed April 2020
Worldometer. (2019), 2020.Population data. https://www.worldometers.info/world-population/india-population/. Accessed April 2020
Xu X, Zhang C (2020). Estimation of ground-level PM2.5 concentration using MODIS AOD and corrected regression model over Beijing, China. PLoS ONE 15(10)
Yong YV, Shafie AA (2016) How much does an asthma-related event cost in a Malaysian suburban hospital? Value Health 19(7):A552
Acknowledgements
Authors thankfully acknowledge Council of Scientific and Industrial Research (CSIR), India, and its constituent laboratory National Environmental Engineering Research Institute (NEERI), and the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2019R1A2C208429411) for supporting the research.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
HB: conceptualisation, methodology, review & editing original draft; SK: software, GIS-visualization; KM & MN: formal analysis, investigation, writing-original draft, graph-visualization; SG, AG, CH, AA: data curation, supervision, draft reviewing; RK: supervision, resources, project coordination. All others have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Bherwani, H., Kumar, S., Musugu, K. et al. Assessment and valuation of health impacts of fine particulate matter during COVID-19 lockdown: a comprehensive study of tropical and sub tropical countries. Environ Sci Pollut Res 28, 44522–44537 (2021). https://doi.org/10.1007/s11356-021-13813-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-021-13813-w