
Abstract
Purpose
Many studies have focused on finding predictors for mild IgAN progression. However, the cases of severe IgAN with a high proportion of global glomerulosclerosis have received inadequate attention.
Methods
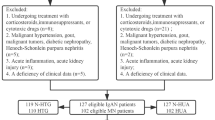
A group of 172 primary IgAN patients with 50–75% global glomerulosclerosis was studied retrospectively between April 2007 and October 2017. Patients were divided into three groups according to the serum triglyceride tertiles: < 1.42 µmol/L (Group 1), 1.42–2.29 µmol/L (Group 2), and > 2.29 µmol/L (Group 3). Groups 1 and 2 comprised non-hypertriglyceridemia subjects, while Group 3 was defined as the hypertriglyceridemia (HTG) group. The patients were followed for 4–96 months (median 39.43 months). The study end point was defined as a 50% decline in estimated glomerular filtration rate (eGFR) or ESRD.
Results
A high proportion of global glomerulosclerosis is not absolutely correlated with severe clinical features and poor renal outcome. In our retrospective observation, eGFR decreased by less than 10% of the baseline during follow-up in 43.6% of the patients. However, in our patients with HTG, the cumulative renal survival rate was significantly lower compared to those without HTG. Multivariate Cox regression analysis also showed that triglyceride is an independent predictor of poor renal outcomes. Furthermore, in the HTG group, the cumulative renal survival rates were higher in patients treated with Tripterygium wilfordii Hook F (TwHF) compared to those without TwHF.
Conclusions
A high proportion of global glomerulosclerosis combined with HTG at biopsy have better predictive validity for the disease progression of IgAN than global glomerulosclerosis alone. TwHF may partially affect the renal outcome of severe IgAN with HTG, and this may relate to its regulation of lipid metabolism and immunoinflammatory response.


Similar content being viewed by others


References
Li LS, Liu ZH (2004) Epidemiologic data of renal diseases from a single unit in China: analysis based on 13,519 renal biopsies. Kidney Int 66(3):920–923
D'Amico G (2000) Natural history of idiopathic IgA nephropathy: role of clinical and histological prognostic factors. Am J Kidney Dis 36(2):227–237
Moriyama T et al (2014) Prognosis in IgA nephropathy: 30-year analysis of 1012 patients at a single center in Japan. PLoS ONE 9(3):e91756
Coppo R (2017) Clinical and histological risk factors for progression of IgA nephropathy: an update in children, young and adult patients. J Nephrol 30(3):339–346
Knoop T et al (2017) Long-term outcome in 145 patients with assumed benign immunoglobulin a nephropathy. Nephrol Dial Transplant 32(11):1841–1850
Walsh M et al (2010) Histopathologic features aid in predicting risk for progression of IgA nephropathy. Clin J Am Soc Nephrol 5(3):425–430
Syrjanen J, Mustonen J, Pasternack A (2000) Hypertriglyceridaemia and hyperuricaemia are risk factors for progression of IgA nephropathy. Nephrol Dial Transplant 15(1):34–42
Yoshida T et al (2008) Risk factors for progression in patients with early-stage chronic kidney disease in the Japanese population. Intern Med 47(21):1859–1864
Zhu X et al (2017) Tubular atrophy/interstitial fibrosis scores of Oxford classification combined with proteinuria level at biopsy provides earlier risk prediction in lgA nephropathy. Sci Rep 7(1):1100
Tsuruya K et al (2017) Association of hypertriglyceridemia with the incidence and progression of chronic kidney disease and modification of the association by daily alcohol consumption. J Ren Nutr 27(6):381–394
Wyatt RJ, Julian BA (2013) IgA nephropathy. N Engl J Med 368(25):2402–2414
National Kidney F (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39(1):S1–266
Working Group of the International Ig, ANN et al (2009) The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int 76(5):534–545
Trimarchi H et al (2017) Oxford classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group. Kidney Int 91(5):1014–1021
Woo KT et al (2016) 30-year follow-up study of IgA nephritis in a Southeast Asian population: an evaluation of the Oxford histological classification. Clin Nephrol 86(11):270–278
Peng W et al (2019) Crescents and global glomerulosclerosis in Chinese IgA nephropathy patients: a five-year follow-up. Kidney Blood Press Res 44(1):103–112
Lee H et al (2014) Long-term prognosis of clinically early IgA nephropathy is not always favorable. BMC Nephrol 15:94
Ruan Y et al (2018) Clinicopathological characteristics, role of immunosuppressive therapy and progression in IgA nephropathy with hyperuricemia. Kidney Blood Press Res 43(4):1131–1140
Maeda K et al (2013) Glomerular tip adhesions predict the progression of IgA nephropathy. BMC Nephrol 14:272
Nguyen C et al (2019) Higher serum galactose-deficient immunoglobulin A1 concentration is associated with stronger mesangial cellular inflammatory response and more severe histologic findings in immunoglobulin A nephropathy. Clin Kidney J 12(2):232–238
He L et al (2017) Characteristics of lipid metabolism including serum apolipoprotein M levels in patients with primary nephrotic syndrome. Lipids Health Dis 16(1):167
Kandasamy N, Ashokkumar N (2014) Renoprotective effect of myricetin restrains dyslipidemia and renal mesangial cell proliferation by the suppression of sterol regulatory element binding proteins in an experimental model of diabetic nephropathy. Eur J Pharmacol 743:53–62
Szeto HH et al (2016) Protection of mitochondria prevents high-fat diet-induced glomerulopathy and proximal tubular injury. Kidney Int 90(5):997–1011
Yang W et al (2018) Ectopic lipid accumulation: potential role in tubular injury and inflammation in diabetic kidney disease. Clin Sci (Lond) 132(22):2407–2422
Wen J et al (2017) Association of the TG/HDL-C and Non-HDL-C/HDL-C ratios with chronic kidney disease in an adult Chinese population. Kidney Blood Press Res 42(6):1141–1154
Hsieh MH et al (2017) Fasting sugar, blood pressure, and uric acid are factors related to positive proteinuria and an impaired eGFR. J Chin Med Assoc 80(12):782–789
Zaman SB et al (2018) Plasma triglycerides as a risk factor for chronic kidney disease in type 2 diabetes mellitus: evidence from northeastern Thailand. Diabet Res Clin Pract 138:238–245
De Cosmo S et al (2016) Predictors of chronic kidney disease in type 2 diabetes: a longitudinal study from the AMD Annals initiative. Medicine 95(27):e4007 (Baltimore)
Low S et al (2016) Onset and progression of kidney disease in type 2 diabetes among multi-ethnic Asian population. J Diabet Complicat 30(7):1248–1254
Lanktree MB et al (2018) HDL cholesterol, LDL cholesterol, and triglycerides as risk factors for CKD: a Mendelian Randomization Study. Am J Kidney Dis 71(2):166–172
Liu J et al (2017) Serum C3 and renal outcome in patients with primary focal segmental glomerulosclerosis. Sci Rep 7(1):4095
Suzuki H et al (2013) Fluctuation of serum C3 levels reflects disease activity and metabolic background in patients with IgA nephropathy. J Nephrol 26(4):708–715
Moriyama T et al (2011) Comparison of steroids and angiotensin receptor blockers for patients with advanced IgA nephropathy and impaired renal function. Am J Nephrol 34(3):233–240
Tan L et al (2018) Combined immunosuppressive treatment may improve short-term renal outcomes in Chinese patients with advanced IgA nephropathy. Kidney Blood Press Res 43(4):1333–1343
Sarcina C et al (2016) Changes in proteinuria and side effects of corticosteroids alone or in combination with azathioprine at different stages of IgA nephropathy. Clin J Am Soc Nephrol 11(6):973–981
Tesar V et al (2015) Corticosteroids in IgA nephropathy: a retrospective analysis from the VALIGA Study. J Am Soc Nephrol 26(9):2248–2258
Chen YZ et al (2010) Meta-analysis of Tripterygium wilfordii Hook F in the immunosuppressive treatment of IgA nephropathy. Intern Med 49(19):2049–2055
Luo L, Yang T (2016) Triptolide inhibits the progression of atherosclerosis in apolipoprotein E(-)/(-) mice. Exp Ther Med 12(4):2307–2313
Wang W (2018) Different doses of Tripterygium glycosides in the treatment of diabetic nephropathy: effects on blood lipids. Kidney Blood Press Res 43(3):931–937
Wang X et al (2014) Anti-inflammatory effects of triptolide by inhibiting the NF-kappaB signalling pathway in LPS-induced acute lung injury in a murine model. Mol Med Rep 10(1):447–452
He L et al (2015) Anti-inflammatory effects of triptolide on IgA nephropathy in rats. Immunopharmacol Immunotoxicol 37(5):421–427
Hong Y et al (2002) Triptolide is a potent suppressant of C3, CD40 and B7h expression in activated human proximal tubular epithelial cells. Kidney Int 62(4):1291–1300
Funding
This work was supported by research grants from the National Natural Science Foundation of China (81870500, 81770714 and 81470947). It was also supported by a research grant (2017JJ2002) from the Natural Science Foundation of Hunan province, and a research grant from Health and Family Planning Commission of Hunan Province (20180922), the Changde Municipal Science and Technology Bureau (2016KZ34).
Author information
Authors and Affiliations
Contributions
Hong Liu and Youming Peng designed the research. Jiayi Wang collected and analyzed the data and wrote the paper. Lingyan He and Danyi Yang collected the data. WenZhe Yan, Xiaofei Peng, and Liyu He contributed some suggestions to the study and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical approval
The studies have been approved by the appropriate institutional research ethics committee and have been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
11255_2019_2371_MOESM1_ESM.docx
Supplementary file1 Components of the composite endpoint in different groups. Data are presented as N (%) or mean ± SD. eGFR estimated glomerular filtration rate, TG triglyceride, HTG hypertriglyceridemia, ESRD end-stage renal disease (DOCX 44 kb)
11255_2019_2371_MOESM2_ESM.docx
Supplementary file2 Baseline clinical characteristics of IgA nephropathy patients with different proportion of gobal glomerulosclerosis. Data are presented as N (%) or mean ± SD. *p < 0.05 was considered significant. aBlood pressure ≥ 140/90 mmHg; bHemoglobin < 110 g/L in females or < 120 g/L in males; serum creatinine in μmol/L to mg/dL, × 0.0113; Blood urea nitrogen in mmol/L to mg/dl, × 2.801. SBP systolic blood pressure, DBP diastolic blood pressure, MAP mean arterial pressure, BUN blood urea nitrogen, UA uric acid, HUA hyperuricemia, Scr serum creatinine, eGFR estimated glomerular filtration rate, TG triglyceride, CHOL total cholesterol, Ig immunoglobulin, C complement, ESR erythrocyte sedimentation rate (DOCX 86 kb)
Rights and permissions
About this article

Cite this article
Wang, J., He, L., Yan, W. et al. The role of hypertriglyceridemia and treatment patterns in the progression of IgA nephropathy with a high proportion of global glomerulosclerosis. Int Urol Nephrol 52, 325–335 (2020). https://doi.org/10.1007/s11255-019-02371-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-019-02371-3