
Abstract
Background
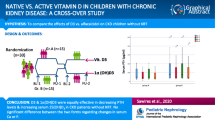
Traditionally, secondary hyperparathyroidism (SHPT) due to low calcitriol synthesis in failing kidneys has been treated with synthetic vitamin D receptor (VDR) activators. Recently, also the importance of low native vitamin D status beyond the issue of SHPT has been recognized in these patients. The aim of this work was to evaluate the effect of cholecalciferol supplementation in haemodialysis patients with low vitamin D serum levels. Another aim was to evaluate dual vitamin D therapy (cholecalciferol supplementation plus paricalcitol) in haemodialysis patients with vitamin D deficiency and concomitant SHPT.
Methods
Ninety clinically stable maintenance haemodialysis patients were included. Supervised cholecalciferol supplementation was administered due to low vitamin D status. Patients with SHPT were also treated with synthetic VDR activator. Two pre hoc subgroups for statistical analysis were formed: patients treated solely with cholecalciferol (N = 34; 5,000 IU once weekly) and patients treated with a combination of cholecalciferol (identical dose, i.e. 5,000 IU/week) plus paricalcitol (N = 34, median dose 10 μg/week). Follow-up visit was scheduled 15 weeks later. Serum concentrations of calcidiol (25-D), parathyroid hormone (PTH) and beta-cross laps (CTX) were assessed at baseline and at follow-up. Serum calcium, phosphate and alkaline phosphatase (ALP) were monitored monthly. Only non-calcium gastrointestinal phosphate binders were administered. Dialysate calcium was 1.5 mmol/L in all patients, and no oral calcium-containing preparations were prescribed. Depending on data distribution, parametric or nonparametric statistical methods were used for comparison within each group (i.e. baseline vs. follow-up data) as well as between groups.
Results
In the whole group of 90 patients, mean baseline 25-D serum level was 20.3 (standard deviation 8.7) nmol/L, and it increased to 66.8 (19) nmol/L (p < 0.0001) after supplementation. In both preformed subgroups, the effect of vitamin D supplementation was almost identical. In cholecalciferol monotherapy, 25-D levels increased from 18.4 (8.2) to 68.6 (21.2) and in dual vitamin D therapy from 18.4 (5.0) to 67.6 (17.7) nmol/L (both p < 0.0001). In addition, both treatment modalities decreased serum PTH levels importantly: from 21.7 (interquartile range 17.3; 35.4) to 18.1 pmol/L (15.3; 24.7) in monotherapy (p = 0.05) and from 38.6 (31.8; 53.3) to 33.9 pmol/L (26.1; 47.5) in dual vitamin D therapy (p = 0.01). Serum calcium, phosphate, ALP and CTX did not change. We have not observed any episode of hypercalcemia in any subject during the whole period of follow-up. At baseline, slightly lower 25-D levels were observed in diabetic than in non-diabetic patients. This difference disappeared after substitution. Vitamin D status and its changes were not related to the patient’s age.
Conclusion
Low 25-D levels were very common in haemodialysis patients. They were safely and effectively corrected with supervised low-dose cholecalciferol supplementation. In patients with higher baseline PTH levels, dual vitamin D therapy (cholecalciferol plus paricalcitol) was safely and effectively used.

Similar content being viewed by others

References
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–281
González EA, Sachdeva A, Oliver DA, Martin KJ (2004) Vitamin D insufficiency and deficiency in chronic kidney disease. A single center observational study. Am J Nephrol 24:503–510
Armas LAG, Andukuri R, Barger-Lux J, Heaney RP, Lund R (2012) 25-Hydroxyvitamin D response to cholecalciferol supplementation in hemodialysis. Clin J Am Soc Nephrol 7:1428–1434
Tokmak F, Quack I, Schieren G, Sellin L, Rattensperger D, Letz TH, Weiner SM, Rump LC (2008) High-dose cholecalciferol to correct vitamin D deficiency in haemodialysis patients. Nephrol Dial Transplant 23:4016–4020
Jones G (2010) Why dialysis patients need combination therapy with both cholecalciferol and a calcitriol analog? Semin Dial 23:239–243
Michaud J, Naud J, Ouimet D, Demers C, Petit JL, Leblond FA, Bonnardeaux A, Gascon-Barre M, Pichette V (2010) Reduced hepatic synthesis of calcidiol in uremia. J Am Soc Nephrol 21:1488–1497
Jean G, Vanel T, Terrat JC, Chazot C (2010) Prevention of secondary hyperparathyroidism in hemodialysis patients: the key role of native vitamin D supplementation. Hemodial Int 14:486–491
London GM, Guerin AP, Verbeke FH, Pannier B, Boutouyrie P, Marchais SJ, Metivier F (2007) Mineral metabolism and arterial functions in end-stage renal disease: potential role of 25-hydroxyvitamin D deficiency. J Am Soc Nephrol 18:613–620
Anand S, Chertow GM, Johansen KL, Grimes B, Darlymple LS, Kaysen A, Kurela Tamura M (2013) Vitamin D deficiency and mortality in patients receiving dialysis: the Comprehensive Dialysis Study. J Ren Nutr 23:422–427
Drechsler C, Verduijn M, Pilz S, Dekker FW, Krediet RT, Ritz E, Wanner C, Boeschoten EW, Brandenburg V, for the NECOSAD Study Group (2011) Vitamin D status and clinical outcomes in incident dialysis patients: results from the NECOSAD study. Nephrol Dial Transplant 26:1024–1032
Pilz S, Tomaschitz A, Friedl C, Amrein K, Drechsler C, Ritz E, Boehm BO, Grammer TB, Maerz W (2011) Vitamin D status and mortality in chronic kidney disease. Nephrol Dial Transplant 26:3603–3609
Taskapan H, Wei M, Oreopoulos DG (2006) 25(OH) Vitamin D3 in patients with chronic kidney disease and those on dialysis: rediscovering its importance. Int Urol Nephrol 38:323–329
Kandula P, Dobre M, Schold JD, Scheiber MJ, Mehrotra R, Navaneethan SD (2011) Vitamin D supplementation in chronic kidney disease: a systematic review and meta-analysis of observational studies and randomized controlled trials. Clin J Am Soc Nephrol 6:50–62
Szeto CC, Kam-Tao Li P (2009) The use of vitamin D analogues in chronic kidney diseases: possible mechanisms beyond bone and mineral metabolism. NDT Plus. doi:10.1093/ndtplus/sfp034
Melamed ML, Thadhani RI (2012) Vitamin D therapy in chronic kidney disease and end stage renal disease. Clin J Am Soc Nephrol 7:358–365
Nigwekar SU, Bhan I, Thadhani R (2012) Ergocalciferol and cholecalciferol in CKD. Am J Kidney Dis 60:139–156
Moorthi RN, Kandula P, Moe SM (2011) Optimal vitamin D, calcitriol and vitamin D analog replacement in chronic kidney disease: to D or not to D: that is the question. Curr Opin Nephrol Hypertens 20:354–359
Vondracek SF, Hoody DW (2011) Combination vitamin D therapy in stage 5 chronic kidney disease. Ann Pharmacother 45:1011–1015
Ravani P, Malberti F, Tripepi G, Pecchini P, Cutrupi S, Pizzini P, Mallamaci F, Zoccali C (2008) Vitamin D levels and patient outcome in chronic kidney disease. Kidney Int 75:88–95
Marckmann P, Agerskov H, Thineshkumar S, Bladbjerg EM, Sidelmann JJ, Jespersen J, Nybo M, Rasmussen LM, Hansen D, Scholze A (2012) Randomized controlled trial of cholecalciferol supplementation in chronic kidney disease patients with hypovitaminosis D. Nephrol Dial Transplant 27:3523–3531
Delanaye P, Weeker L, Warling X, Moonen M, Smelten N, Médart L, Krzesinski JM, Cavalier E (2013) Cholecalciferol in haemodialysis patients: a randomized, double-blind, proof-of-concept and safety study. Nephrol Dial Transplant 28:1779–1786
Gardham C, Stevens PE, Delaney MP, LeRoux M, Coleman A, Lamb EJ (2010) Variability of parathyroid hormone and other markers of bone mineral metabolism in patients receiving hemodialysis. Clin J Am Soc Nephrol 5:1261–1267
Sardiwal S, Gardham C, Coleman AE, Stevens PE, Delaney MP, Lamb EJ (2012) Bone-specific alkaline phosphatase concentrations are less variable than those of parathyroid hormone in stable hemodialysis patients. Kidney Int 82:100–105
Matias PJ, Jorge C, Ferreira C, Borges M, Aires I, Amaral T, Gil C, Cortez J, Ferreira A (2010) Cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac dimension parameters. Clin J Am Soc Nephrol 5:905–911
Saab G, Young DO, Gincherman Y, Giles K, Norwood K, Coyne DW (2007) Prevalence of vitamin D deficiency and the safety and effectiveness of monthly ergocalciferol in haemodialysis patients. Nephron Clin Pract 105:132–138
Armas LAG, Zena M, Lund R, Heaney RP (2013) Calcium absorption response to cholecalciferol supplementation in haemodialysis. Clin J Am Soc Nephrol 8:1003–1008
Braunlin W, Zhorow E, Guo A, Apruzzese W, Xu Q, Hook P, Smisek DL, Mandeville HM, Holmes-Farley SR (2002) Bile acid binging to sevelamer HCl. Kidney Int 62:611–619
Jean G, Souberbielle JC, Chazot C (2009) Monthly cholecalciferol administration in haemodialysis patients: a simple and efficient strategy for vitamin D supplementation. Nephrol Dial Transplant 24:3799–3805
Massart A, Debelle FD, Racape J, Gervy C, Husson C, Dhaene M, Wissing KM, Nortier JL (2014) Biochemical parameters after cholecalciferol repletion in hemodialysis: Results from the VitaDial randomized trial. Am J Kidney Dis. doi:10.1053/j.ajkd.2014.04.020
Acknowledgments
This study was supported by Research Project NT/11355-4/2010 Ministry of Health of the Czech Republic.
Conflict of interest
S.D.S. served as speaker for Amgen (Czech Republic) and Abbvie (Czech Republic). There is no conflict of interest in co-authors of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dusilová-Sulková, S., Šafránek, R., Vávrová, J. et al. Low-dose cholecalciferol supplementation and dual vitamin D therapy in haemodialysis patients. Int Urol Nephrol 47, 169–176 (2015). https://doi.org/10.1007/s11255-014-0842-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-014-0842-7