
Abstract
Objectives
Currently available studies show controversial data between the symptoms of the lower urinary tract and the volume of the prostate gland. The objective of the present study is to evaluate the relationship between the score of the lower urinary tract symptoms assessed according to the International Prostate Symptoms Score (IPSS) and the total (TV) and transitional (TZV) zone volume of the prostate and transitional prostate zone index (TZI).
Materials and methods
From 223 men with a mean age of 59.3 years (varying from 50 to 75), the scores of lower urinary tract symptoms, measured by the IPSS and TV and TZV, determined by transrectal ultrasonographies, were obtained. Furthermore, the TZI was determined in all cases by the TZV to TV rate of the prostate. The relationship between TV, TZV, and TZI and the data obtained using the symptoms score was statistically determined.
Results
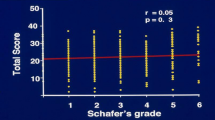
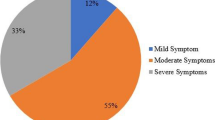
The TV of the prostate were 25.5 ± 10.3, 25.0 ± 9.3, and 28.9 ± 13.5 g in individuals with mild, moderate, and severe symptoms, respectively (P = 0.15). Similarly, there was no significant difference when the TZV (7.6 ± 6.3, 7.6 ± 5.8, and 9.6 ± 6.8 g, respectively; P = 0.22) and the TZI (0.26 ± 0.1, 0.27 ± 0.1, and 0.30 ± 0.1, respectively; P = 0.33) were compared in the groups of men with mild, moderate, and severe symptoms of urinary difficulty. However, the quality of life (QoL) scores presented progressively worse values (1.7 ± 1.3, 3.1 ± 1.4, and 4.4 ± 1.2) as the severity of the lower urinary tract symptoms became worse (P < 0.001). The Pearson correlation coefficient between the TV (r = 0.15; P = 0.02), TZV (r = 0.16; P = 0.02), and the TZI (r = 0.14; P = 0.03) with the prostate symptom scores showed low values although they were positive and statistically significant. The highest correlation was observed when the QoL related to urinary symptoms and symptom scores (r = 0.61; P < 0.001) was analyzed.
Conclusions
A low correlation was found between the score lower urinary tract symptoms assessed by IPSS and the different volumes of the prostate gland (TV, TZV) and prostate TZI, and, on the other hand, an inverse correlation between the intensity of urinary symptoms and QoL, supporting the idea of multifactorial aspects related to the genesis of urinary symptoms in men.




Similar content being viewed by others

References
Shapiro E, Lepor H (1995) Pathophysiology of clinical benign prostatic hyperplasia. Urol Clin North Am 22(2):285–290
Issacs JT, Coffey DS (1989) Etiology and disease process of benign prostatic hyperplasia. Prostate 2:33–50
Guess HA, Arrighi HM, Metter EJ, Fozard JL (1990) Cumulative prevalence of prostatism matches the autopsy prevalence of benign prostatic hyperplasia. Prostate 17(3):241–246
Kirby RS (2000) The natural history of benign prostatic hyperplasia: what have we learned in the last decade? Urology 56(5 suppl 1):3–6
O’Leary MP (2000) LUTS, ED, QOL: alphabet soup or real concerns to aging men? Urology 56(5A):7–11
Girmam CJ, Jacobsen SJ, Guess HA, Oesterling JE, Chute CG, Panser LA, Lieber MM (1995) Natural history of prostatism: relationship among symptoms, prostate volume and peak urinary flow rate. J Urol 153:1510–1515
Osterling JE, Jacobsen SJ, Chute CG, Guess HA, Girman CJ, Panser LA, Lieber MM (1993) Serum prostate specific antigen in a community-based population of healthy men: establishment of age-specific reference ranges. JAMA 270(7):860–864
Bosch JL, Kranse HR, Van Mastrigt R, Schröder FH (1995) Reasons for the weak correlation between prostate volume and urethral resistence parameters in patients with prostatism. J Urol 153(3 pt 1):689–693
Barry MJ, Cockett AT, Holtgrewe HL, McConnell JD, Sihelnik SA, Winfield HN (1993) Relationship of symptoms of prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. J Urol 150(2 Pt 1): 351–358
McNeal JE (1988) The prostate gland: morphology and pathobiology. Monogr Urol 9:36–41
Barry MJ, Fowler FJ, O′Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, Cockett ATK (1992) Measurement Committee of American Urological Association: The American Urological Association symptom index for benign prostate hyperplasia. J Urol 148(5):1549–1557
International Consensus Committee (1993) Recommendations of the International Consensus Committee. In: Cockett ATK, Khoury S, Aso Y et al. (eds) Proceedings of the 2nd International Consultation on Benign Prostate Hyperplasia (BPH). Jersey, Channel Islands, Scientific Communication International, p. 556–564
Yoshimura K, Arai Y, Ichioka K, Terada N, Matsuta Y, Okubo K (2002) Symptom-specific quality of life in patients with benign prostatic hyperplasia. Int J Urol 9:485–490
Desgrandchamps F, Droupy S, Irani J, Saussine C, Comenducci A (2006) Effects of dutasteride on the symptoms of benign prostatic hyperplasia, and patient quality of life and discomfort, in clinical practice. Br J Urol Int 98:83–88
Gacci M, Bartoletti R, Figlioli S, Sarti FE, Eisner B, Bodd V, Rizzo M (2003) Urinary symptoms, quality of life and sexual function in patients with benign prostatic hypertrophy before and after prostatectomy: a prospective study. Br J Urol Int 91:196–200
Sukov RJ, Scardino PT, Sample WF, Winter J, Confer DJ (1977) Computed tomography and transabdominal ultrasound in the evaluation of the prostate. J Comput Assist Tomogr 1(3):281–289
Roehrborn CG, Bartsch G, Kirby R, Andriole G, Boyle P, De La Rosette J, Perrin P, et al (2001) Guidelines for the diagnosis and treatment of benign prostatic hyperplasia: a comparative international overview. Urology 58:642–650
Chute CG, Guess HA, Panser LA, Johnson CL, Jacobsen SJ, Oesterling JE, Lieber MM (1993) The non-relationship of urinary symptoms prostate volume and uroflow in a population based sample of men. J Urol 149:356
Overland GB, Vatten L, Rhodes T, De Muro C, Jaconbsen G, Vada K, Angelsen A, et al (2001) Lower urinary tract symptom prostate volume and uroflow in Norwegian community men. Eur Urol 39(1):36–41
Greene DR, Egawa S, Hellerstein DK, Scardino PT (1990) Sonographic measurements of transition zone of prostate in men with and without benign prostatic hyperplasia. Urology 36(4):293–299
Kaplan AS, Te AE, Pressler LB, Olsson CA (1995) Transition zone index as a method of assessing benign prostatic hyperplasia: correlation with symptoms, urine flow and detrusor pressure. J Urol 154(5):1764–1769
Kaplan AS, Reis RB, Staimen VB, Te AE (1998) Is the ratio of transition zone to total prostate volume in their Caucasian Africa-American men than in their Caucasian or hispanic counterparts? Br J Urol 82(6):804–807
Caine M, Pfau A, Perlberg S (1976) The use of alpha-adrenergic blockers in benign prostatic obstruction. Br J Urol 48(4):255–263
Hutch JA, Rambo ON Jr (1970) A study of the anatomy of the prostate, prostatic urethra and the urinary sphincter system. J Urol 104(3):443–452
Grayhack JT, McVary KT, Kozlowski JM (2002) Benign prostatic hyperplasia. In: Gllenwater J, Grayhack JT, Howards S (eds) Adult and pediatric urology. St Louis, Mosby, 2, pp. 1401–1470
Gotoh M, Kamihira O, Kinukawa T, Ono Y, Ohshima S, Origasa H (2005) Comparison of tamsulosin and naftopidil for efficacy and safety in the treatment of benign prostatic hyperplasia: a randomized controlled trial. Br J Urol Inter 96(4):581
Haltbakk J, Hanestad BR, Hunskaar S (2005) How important are men lower urinary tract symptoms (LUTS) and their impact on the quality of life (QoL). Qual Life Res Sep 14(7):1733–1741
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Franciosi, M., Koff, W.J. & Rhoden, E.L. Correlation between the total volume, transitional zone volume of the prostate, transitional prostate zone index and lower urinary tract symptoms (LUTS). Int Urol Nephrol 39, 871–877 (2007). https://doi.org/10.1007/s11255-006-9148-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-006-9148-8