
Abstract
Objectives
To evaluate the diagnostic performance of 14-core repeat biopsy protocol and the impact of prior biopsy scheme on repeat prostate biopsy group.
Methods
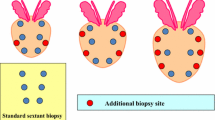
211 patients had repeat biopsy using 14-core protocol consisting of 10-core peripheral zone (classical sextant+4 lateral peripheral cores) and 4-core transitional zone (TZ) biopsies. The diagnostic yield was determined both in patients who had previously undergone sextant or 10-core biopsy protocol.
Results
Overall cancer detection rate was 25.6%. 14-core biopsy technique detected cancer in 36.1 and 18.7% of the patients who had a previous sextant biopsy and 10-core biopsy protocol, respectively (P = 0.005). Patients with and without high-grade prostatic intraepithelial neoplasia (HGPIN) in the previous sextant biopsy had 56.5 and 28.3% cancer detection rates on the subsequent extended biopsy, respectively (P = 0.017) Patients who had previous 10-core biopsy with and without HGPIN revealed 22.9 and 17.2% cancer detection rates, respectively (P = 0.465) Additional four lateral peripheral cores detected 33% (3/30) and 17% (4/24) of cancers in patients with previous sextant and 10-core biopsy, respectively. 3.7% of the patients had tumor only in the TZ and none of them had prior extended biopsy.
Conclusions
The yield of extended 14-core repeat biopsy protocol was higher in patients with previous negative sextant biopsy compared to the patients with previous negative 10-core biopsy. HGPIN history found on previous sextant biopsy was a strong cancer predictor on repeat biopsy; same was not true for the patients with previous 10-core biopsy. The yield of lateral peripheral cores and TZ biopsies were lower in patients with prior negative extended biopsy.
Similar content being viewed by others

References
Hodge KK, McNeal JE, Terris MK, Stamey TA (1989) Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J Urol 142:71–74
Rabbani F, Stroumbakis N, Kava BR, Cookson M, Fair WR (1998) Incidence and clinical significance of false-negative sextant prostate biopsies. J Urol 159:1247–1251
Presti JC Jr (2003) Prostate biopsy: how many cores are enough? Urol Oncol 21(2):135–143
Eskew LA, Bare RL, McCullough DL (1997) Systematic 5 region prostate biopsy is superior to sextant method diagnosing carcinoma of the prostate. J Urol 157:199–202
Eskicorapci SY, Baydar DE, Akbal C, Sofikerim M, Günay M, Ekici S, Ozen H (2004) An extended 10-core transrectal ultrasonography-guided prostate biopsy protocol improves the detection of prostate cancer. Eur Urol 45(4):444–448
Eskicorapci SY, Guliyev F, Akdogan B, Dogan HS, Ergen A, Ozen H (2005) Individualization of the biopsy protocol according to the prostate gland volume for prostate cancer detection. J Urol 173:1536–1539
Djavan B, Ravery V, Zlotta A, Dobronski P, Dobrovits M, Fakhari M et al (2001) Prospective evaluation of prostate cancer detected on biopsies 1, 2, 3 and 4: When should we stop? J Urol 166:1679–1684
Borboroglu PG, Comer SW, Riffenburgh RH, Amling CL (2000) Extensive repeat transrectal ultrasound guided prostate biopsy in patients with previous benign sextant biopsies. J Urol 163:158–161
Stewart CS, Leibovich BC, Weaver AL, Lieber MM (2001) Prostate cancer diagnosis using a saturation needle biopsy technique after previous negative sextant biopsies. J Urol 166:86–90
Carter HB, Epstein JI, Chan DW, Fozard JL, Pearson JD (1997) Recommended prostate-specific antigen testing intervals for the detection of curable prostate cancer. JAMA 277:1456
Hong YM, Lai FC, Chon CH, McNeal JE, Presti JC Jr (2004) Impact on prior biopsy scheme on pathological features of cancers detected on repeat biopsies. Urol Oncol 22:7–11
Chon CH, Lai FC, McNeal JE, Presti JC (2002) Use of extended systematic sampling in patients with a prior negative prostate needle biopsy. J Urol 167:2457–2461
Babaian RJ, Toi A, Kamoi K, Troncoso P, Sweet J, Evans R et al (2000) A comparative analysis of sextant and an extended 11-core multisite directed biopsy strategy. J Urol 163:152–156
Applewhite JC, Matlaga BR, McCullough DL (2002) Results of the 5 region prostate biopsy method: the repeat biopsy population. J Urol 168:500–504
Eskicorapci SY, Karabulut E, Türkeri L, Baltaci S, Cal C, Toktas G et al (2005) Validation of 2001 Partin tables in Turkey: a multicenter study. Eur Urol 47:185–188
Herawi M, Kahane H, Cavallo C, Epstein JI (2006) Risk of prostate cancer on first re-biopsy within 1 year following a diagnosis of high grade prostatic intraepithelial neoplasia is related to the number of cores sampled. J Urol 175:121–124
Lopez-Corona E, Ohori M, Scardino PT, Reuter VE, Gonen M, Kattan MW (2003) A nomogram for predicting a positive repeat prostate biopsy in patients with a previous negative biopsy session. J Urol 170:1184–1189
Keetch DW, Catalona WJ (1995) Prostatic transition zone biopsies in men with previous negative biopsies and persistently elevated serum prostate specific antigen values. J Urol 154:1795–1799
Lui PD, Terris MK, McNeal JE, Stamey TA (1995) Indications for ultrasound guided transition zone biopsies in the detection of prostate cancer. J Urol 153:1000–1005
Author information
Authors and Affiliations
Corresponding author
Additional information
Take home messages: The 14-core repeat biopsy protocol was superior in patients with previous negative sextant biopsy. HGPIN history on previous sextant biopsy was a strong cancer predictor. Yield of lateral peripheral and TZ biopsies were lower in patients with prior extended biopsy.
Rights and permissions
About this article
Cite this article
Eskicorapci, S.Y., Guliyev, F., Islamoglu, E. et al. The Effect of Prior Biopsy Scheme on Prostate Cancer Detection for Repeat Biopsy Population: Results of the 14-core Prostate Biopsy Technique. Int Urol Nephrol 39, 189–195 (2007). https://doi.org/10.1007/s11255-006-9009-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-006-9009-5