
Abstract
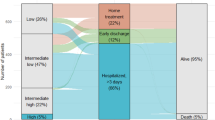
Current guidelines consider outpatient treatment as an option for low-risk pulmonary embolism (PE), and risk assessment tools such as the HESTIA criteria can be used to identify PE patients who could feasibly be treated in an outpatient setting. Little is known about what proportion of patients in daily care this would comprise, and, in these patients, outcome data outside of clinical trials are scarce. To assess the proportion of PE patients receiving outpatient early discharge or in-hospital therapy, evaluate differences in patient characteristics between these subgroups and to assess clinical outcomes at 6 months. Monocentric, retrospective cohort study in 439 consecutive patients undergoing outpatient, early-discharge or in-hospital treatment for PE. Outcome data on recurrent VTE, pulmonary hypertension or death were collected from routine follow-up visits 6 months after VTE diagnosis. PE patients were treated as outpatient (OP; n = 49; 11.2 %); early-discharge (ED; n = 62; 14.1 %) or in-hospital (IH; n = 328; 74.7 %). Median duration of hospital stay in the ED and IH groups were 1 (IQR: 1) day and 9 (IQR: 7) days, respectively. Outcome event rates at 6 months were 3.9 % for recurrent VTE (95 % CI 2.3–6.1, similar between groups), 5.2 % for pulmonary hypertension (95 % CI 3.3–7.8, similar between groups) and 10.7 % for mortality (95 % CI 8.0–14.0). Mortality was significantly higher in IH patients (14.0 %; 95 % CI 10.5–18.3) compared to OP (0 %; 95 % CI 0.0–7.3) or ED (1.6 %; 95 % CI 0.0–8.7) patients. Mortality risk factors were high-risk ESC category (OR: 5.7), paraneoplastic VTE (OR: 3.0), need for oxygen supplementation (OR: 5.2), diabetes (OR: 2.5), age (OR per additional year: 1.1) and elevated INR (OR per 0.1 point increase: 1.5). No difference in the treatment groups for pulmonary hypertension during follow-up was found. Independent risk factors were thrombophilia (OR: 8.43), signs of right ventricular strain in baseline ECG (OR: 6.64) or echocardiography (RVESP > 40 mmHg OR: 2.99). 32 % of the OP or ED patients had at least one criterion of the HESTIA score that would have excluded them from outpatient treatment. In daily care, treating PE in an almost exclusively outpatient setting seems feasible and safe for up to 25 % of all PE patients. The HESTIA criteria seem to exclude up to 30 % of patients for whom outpatient or early-discharge treatment seems feasible and safe.

Similar content being viewed by others


References
Kearon C, Akl EA, Comerota AJ et al (2012) Antithrombotic therapy for VTE disease antithrombotic therapy and prevention of thrombosis, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141:e419S–e494S. doi:10.1378/chest.11-2301
Blättler W, Gerlach H, Hach-Wunderle et al (2010) Diagnostik und Therapie der Venenthrombose und der Lungenembolie. Vasa 39:1–39
Stein EM, Carrelli A, Young P et al (2013) Bariatric surgery results in cortical bone loss. J Clin Endocrinol Metab 98:541–549. doi:10.1210/jc.2012-2394
Lankeit M, Konstantinides S (2012) Is it time for home treatment of pulmonary embolism? Eur Respir J. doi:10.1183/09031936.00216811
Husted SE, Nielsen HK (2010) Treatment of pulmonary embolism at home? Thromb Res 126:3–4. doi:10.1016/j.thromres.2009.12.020
Tapson VF, Huisman MV (2007) Home at last? Early discharge for acute pulmonary embolism. Eur Respir J 30:613–615. doi:10.1183/09031936.00098007
Konstantinides S, Geibel A, Olschewski M et al (1997) Association between thrombolytic treatment and the prognosis of hemodynamically stable patients with major pulmonary embolism: results of a multicenter registry. Circulation 96:882–888
Kucher N, Rossi E, De Rosa M, Goldhaber SZ (2005) Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med 165:1777–1781. doi:10.1001/archinte.165.15.1777
Aujesky D, Roy P-M, Verschuren F et al (2011) Outpatient versus inpatient treatment for patients with acute pulmonary embolism: an international, open-label, randomised, non-inferiority trial. Lancet 378:41–48. doi:10.1016/S0140-6736(11)60824-6
Jiménez D, Aujesky D, Moores L et al (2010) Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med 170:1383–1389. doi:10.1001/archinternmed.2010.199
Venetz C, Jiménez D, Mean M, Aujesky D (2011) A comparison of the original and simplified Pulmonary Embolism Severity Index. Thromb Haemost 106:423–428. doi:10.1160/TH11-04-0263
Zondag W, Mos ICM, Creemers-Schild D et al (2011) Outpatient treatment in patients with acute pulmonary embolism: the Hestia Study. J Thromb Haemost 9:1500–1507. doi:10.1111/j.1538-7836.2011.04388.x
Zondag W, den Exter PL, Crobach MJT et al (2013) Comparison of two methods for selection of out of hospital treatment in patients with acute pulmonary embolism. Thromb Haemost 109:47–52. doi:10.1160/TH12-07-0466
Zondag W, Vingerhoets LMA, Durian MF et al (2013) Hestia criteria can safely select patients with pulmonary embolism for outpatient treatment irrespective of right ventricular function. J Thromb Haemost 11:686–692. doi:10.1111/jth.12146
Zondag W, Hiddinga BI, Crobach MJT et al (2013) Hestia criteria can discriminate high- from low-risk patients with pulmonary embolism. Eur Respir J 41:588–592. doi:10.1183/09031936.00030412
Torbicki A, Perrier A, Konstantinides S et al (2008) Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 29:2276–2315. doi:10.1093/eurheartj/ehn310
Schwarz T, Schmidt B, Beyer J et al (2001) Eligibility for home treatment of deep vein thrombosis: a prospective study in 202 consecutive patients. J Vasc Surg 34:1065–1070. doi:10.1067/mva.2001.118821
Schellong SM, Schwarz T, Kropp J et al (1999) Bed rest in deep vein thrombosis and the incidence of scintigraphic pulmonary embolism. Thromb Haemost 82(Suppl 1):127–129
Schwarz T, Schmidt B, Schmidt B, Schellong SM (2002) Interobserver agreement of complete compression ultrasound for clinically suspected deep vein thrombosis. Clin Appl Thromb Hemost 8:45–49
Van Rossum AB, van Houwelingen HC, Kieft GJ, Pattynama PM (1998) Prevalence of deep vein thrombosis in suspected and proven pulmonary embolism: a meta-analysis. Br J Radiol 71:1260–1265. doi:10.1259/bjr.71.852.10318998
Girard P, Musset D, Parent F et al (1999) High prevalence of detectable deep venous thrombosis in patients with acute pulmonary embolism. Chest 116:903–908
Bell EJ, Selvin E, Lutsey PL et al (2013) Glycemia (hemoglobin A1c) and incident venous thromboembolism in the Atherosclerosis Risk in Communities cohort study. Vasc Med 18:245–250. doi:10.1177/1358863X13506764
Glynn RJ, Danielson E, Fonseca FAH et al (2009) A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med 360:1851–1861. doi:10.1056/NEJMoa0900241
Oren E, Smith NL, Doggen CJM et al (2006) Body mass index and the risk of venous thrombosis among postmenopausal women. J Thromb Haemost 4:2273–2275. doi:10.1111/j.1538-7836.2006.02119.x
Kim NH, Lang IM (2012) Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir Rev 21:27–31. doi:10.1183/09059180.00009111
Vanni S, Nazerian P, Pepe G et al (2011) Comparison of two prognostic models for acute pulmonary embolism: clinical vs. right ventricular dysfunction-guided approach. J Thromb Haemost 9:1916–1923. doi:10.1111/j.1538-7836.2011.04459.x
Levitan N, Dowlati A, Remick SC et al (1999) Rates of initial and recurrent thromboembolic disease among patients with malignancy versus those without malignancy. Risk analysis using Medicare claims data. Medicine (Baltimore) 78:285–291
Hogg K, Hinchliffe E, Haslam S et al (2013) Predicting short term mortality after investigation for venous thromboembolism. Thromb Res 131:e141–e146. doi:10.1016/j.thromres.2013.01.030
Aujesky D, Obrosky DS, Stone RA et al (2005) Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med 172:1041–1046. doi:10.1164/rccm.200506-862OC
Conflict of interest
None of the authors declared a conflict of interest with regard to the presented data. No financial or editorial support was obtained for this study or the writing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Werth, S., Kamvissi, V., Stange, T. et al. Outpatient or inpatient treatment for acute pulmonary embolism: a retrospective cohort study of 439 consecutive patients. J Thromb Thrombolysis 40, 26–36 (2015). https://doi.org/10.1007/s11239-014-1141-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-014-1141-y