
Abstract
Objectives
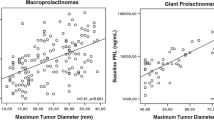
Prolactin (PRL)-secreting macroadenomas usually measure between 10 and 40 mm. Giant (adenoma size ≥40 mm) PRL-tumors are not common, and larger prolactinomas (maximal diameter ≥60 mm) are rare, and their management outcomes have not been well characterized.
Methods
We have identified 18 subjects (16 men, 2 females) with giant PRL-adenomas (size ≥60 mm; PRL > 1000 ng/ml) and summarized their characteristics and response to treatment.
Results
Mean age was 36.3 ± 13.5 years (range 12–59 years). Mean adenoma size was 71.8 ± 10.2 mm (60–92 mm). Complaints at presentation included headaches in 11 patients, visual deterioration in 9, sexual dysfunction in 9 males, and behavioral changes in two. Fourteen (78 %) had visual field defects. Mean PRL at presentation was 28,465 ng/ml (range 1300–270,000). All patients were treated with cabergoline (3.9 ± 2.0 mg/week), except for one who received bromocriptine. Treatment achieved PRL normalization in 11/18 patients within a median interval of 20 months. Visual improvement occurred in 12/14 patients with pre-treatment visual abnormalities. Nine patients underwent surgery (transsphenoidal, 7; transcranial, 2). None of the seven patients with elevated PRL before surgery achieved remission post-operatively. After a follow-up of 7.8 ± 5.1 years, 15/18 patients had significant adenoma shrinkage. Eleven patients are normoprolactinemic, 3 are partially controlled (PRL < 3 × ULN), and 4 remain with significantly elevated PRL. Most patients reported disappearance or improvement of their complaints.
Conclusions
These enormous PRL-adenomas are invasive but respond fairly well to medical treatment. Long-term therapy with high dose cabergoline together with a pituitary surgery in some patients was the key for their successful management, achieving biochemical and clinical remission in most patients.



Similar content being viewed by others


References
Colao A, Sarno AD, Cappabianca P, Briganti F, Pivonello R, Somma CD, Faggiano A, Biondi B, Lombardi G (2003) Gender differences in the prevalence, clinical features and response to cabergoline in hyperprolactinemia. Eur J Endocrinol 148:325–331
Gillman MP, Molitch ME, Lombardi G, Colao A (2006) Advances in the treatment of prolactinomas. Endocr Rev 27:485–534
Maiter D, Delgrange E (2014) Therapy of endocrine disease: the challenges in managing giant prolactinomas. Eur. J. Endocrinol. 170 R:213–227
Shrivastava RK, Arginteanu MS, King WA, Post KD (2002) Giant prolactinomas: clinical management and long-term follow up. J Neurosurg 97:299–306
Corsello SM, Ubertini G, Altomare M, Lovicu RM, Migneco MG, Rota CA, Colosimo C (2003) Giant prolactinomas in men: efficacy of cabergoline treatment. Clin Endocrinol (Oxf) 58:662–670
Shimon I, Benbassat C, Hadani M (2007) Effectiveness of long-term cabergoline treatment for giant prolactinomas: study of 12 men. Eur J Endocrinol 156:225–231
Delgrange E, Raverot G, Bex M, Burman P, Decoudier B, Devuyst F, Feldt-Rasmussen U, Andersen M, Maiter D (2013) Giant prolactinomas in women. Eur J Endocrinol 170:31–38
Espinosa E, Sosa E, Mendoza V, Ramírez C, Melgar V, Mercado M (2016) Giant prolactinomas: are they really different from ordinary macroprolactinomas? Endocrine. doi:10.1007/s12020-015-0791-7
Grozinsky-Glasberg S, Shimon I (2011) Unusual clinical presentations of giant prolactinomas. Pituitary 14:340–344
Grebe SK, Delahunt JW, Feek CM (1992) Treatment of extensively invasive (giant) prolactinomas with bromocriptine. N Z Med J 105:129–131
Tirosh A, Shimon I (2016) Current approach to treatments for prolactinomas. Minerva Endocrinol [Epub ahead of print]
Colao A, Vitale G, Cappabianca P, Briganti F, Ciccarelli A, De Rosa M, Zarrilli S, Lombardi G (2004) Outcome of cabergoline treatment in men with prolactinoma: effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J Clin Endocrinol Metab 89:1704–1711
Tirosh A, Benbassat C, Shimon I (2015) Short-term decline in prolactin concentrations can predict future prolactin normalization, tumor shrinkage, and time to remission in men with macroprolactinomas. Endocr Pract 21:1240–1247
Madsen H, Borges TM, Knox AJ, Michaelis KA, Xu M, Lillehei KO, Wierman ME, Kleinschmidt-DeMasters BK (2011) Giant pituitary adenomas: pathologic-radiographic correlations and lack of role for p53 and MIB-1 labeling. Am J Surg Pathol 35:1204–1213
Deepak D, Daousi C, Javadpour M, MacFarlane IA (2007) Macroprolactinomas and epilepsy. Clin Endocrinol (Oxf) 66:503–507
Brisman MH, Fetell MR, Post KD (1993) Reversible dementia due to macroprolactinoma. Case report. J Neurosurg 79:135–137
Acknowledgments
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Ilan Shimon, has received research grants, consulting and lectureship fees from Novartis and Pfizer. Yona Greenman received research grant from Pfizer, and research grant, travel support and speaker fees from Novartis. Marcello D. Bronstein, is speaker for Ipsen and Novartis, member of steering committees for Chiasma, Ipsen and Novartis. Moises Mercado is a consultant and lecturer for Novartis Oncology and Ipsen. Ernesto Sosa, Victoria Mendoza, Amit Tirosh, Etual Espinosa and Andrea Glezer have no conflicts of interest to declare.
Rights and permissions
About this article

Cite this article
Shimon, I., Sosa, E., Mendoza, V. et al. Giant prolactinomas larger than 60 mm in size: a cohort of massive and aggressive prolactin-secreting pituitary adenomas. Pituitary 19, 429–436 (2016). https://doi.org/10.1007/s11102-016-0723-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-016-0723-4