
Abstract
Introduction
Immunoglobulin (Ig) G4-related hypophysitis is an emerging clinical entity, which is characterized by an elevated serum IgG4 concentration and infiltration of IgG4-positive plasma cells in the pituitary. Although some criteria for its diagnosis have been proposed, they have not been fully established. In particular, differential diagnosis from secondary chronic inflammation including granulomatosis with polyangiitis (GPA) is difficult in some cases. We describe central diabetes insipidus with pituitary swelling exhibiting infiltration of IgG4-positive cells.
Patient
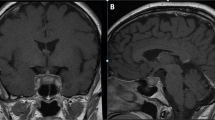
A 43-year-old woman in the remission stage of GPA presented with sudden-onset polyuria and polydipsia. Pituitary magnetic resonance imaging revealed swelling of the anterior and posterior pituitary and stalk, with heterogeneous gadolinium enhancement and disappearance of the high signal intensity of the posterior pituitary. Evaluation of biochemical markers for GPA suggested that the disease activity was well-controlled. Endocrinological examination revealed the presence of central diabetes insipidus and growth hormone deficiency. Pituitary biopsy specimen showed IgG4-positive cells, with a 43 % IgG4+/IgG+ ratio, which met the criteria for IgG4-related hypophysitis. However, substantial infiltration of polymorphonuclear neutrophils with giant cells was also noted, resulting in a final diagnosis of pituitary involvement of GPA.
Conclusion
These results suggest that pituitary involvement of GPA should be taken into account for the differential diagnosis of IgG4-related hypophysitis.



Similar content being viewed by others


References
Shimatsu A, Oki Y, Fujisawa I, Sano T (2009) Pituitary and stalk lesions (infundibulo-hypophysitis) associated with immunoglobulin G4-related systemic disease: an emerging clinical entity. Endocr J 56:1033–1041
Bando H, Iguchi G, Fukuoka H, Taniguchi M, Yamamoto M, Matsumoto R, Suda K, Nishizawa H, Takahashi M, Kohmura E, Takahashi Y (2014) The prevalence of IgG4-related hypophysitis in 170 consecutive patients with hypopituitarism and/or central diabetes insipidus and review of the literature. Eur J Endocrinol 170:161–172
Leporati P, Landek-Salgado MA, Lupi I, Chiovato L, Caturegli P (2011) IgG4-related hypophysitis: a new addition to the hypophysitis spectrum. J Clin Endocrinol Metab 96:1971–1980
Osawa S, Ogawa Y, Watanabe M, Tominaga T (2009) Hypophysitis presenting with atypical rapid deterioration: with special reference to immunoglobulin G4-related disease-case report. Neurol Med Chir (Tokyo) 49:622–625
Hattori Y, Tahara S, Ishii Y, Kitamura T, Inomoto C, Osamura RY, Teramoto A, Morita A (2013) A case of IgG4-related hypophysitis without pituitary insufficiency. J Clin Endocrinol Metab 98:1808–1811
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA (2013) 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 65:1–11
Yi ES, Colby TV (2001) Wegener’s granulomatosis. Semin Diagn Pathol 18:34–46
Woywodt A, Haubitz M, Haller H, Matteson EL (2006) Wegener’s granulomatosis. Lancet 367:1362–1366
Yong TY, Li JY, Amato L, Mahadevan K, Phillips PJ, Coates PS, Coates PT (2008) Pituitary involvement in Wegener’s granulomatousis. Pituitary 11:77–84
Kallenberg CG, Mulder AH, Tervaert JW (1992) Antineutrophil cytoplasmic antibodies: a still growing class of autoantibodies in inflammatory disorders. Am J Med 93:675–682
Hoffman GS, Specks U (1998) Anti-neutrophil cytoplasmic antibodies. Arthritis Rheum 41:1521–1537
Chang SY (2013) IgG4-positive plasma cells in granulomatosis with polyangiitis (Wegener’s): a clinicopathologic and immunohistochemical study on 43 granulomatosis with polyangiitis and 20 control cases. Hum Pathol 44:2432–2437
Ebbo M, Grados A, Bernit E, Vély F, Boucraut J, Harlé JR, Daniel L, Schleinitz N (2012) Pathologies associated with serum IgG4 elevation. Int J Rheumatol 2012:602809
Nishioka H, Shibuya M, Haraoka J (2010) Immunohistochemical study for IgG4-positive plasmacytes in pituitary inflammatory lesions. Endocr Pathol 21:236–241
Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, Arend WP et al (1990) The American College of Rheumatology 1990 criteria for the classification of Wegener’s granulomatosis. Arthritis Rheum 33:1101–1107
Watts R, Lane S, Hanslik T, Hauser T, Hellmich B, Koldingsnes W, Mahr A, Segelmark M, Cohen-Tervaert JW, Scott D (2007) Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann Rheum Dis 66:222–227
Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, Klöppel G, Heathcote JG, Khosroshahi A, Ferry JA, Aalberse RC, Bloch DB, Brugge WR, Bateman AC, Carruthers MN, Chari ST, Cheuk W, Cornell LD, Fernandez-Del Castillo C, Forcione DG, Hamilos DL, Kamisawa T, Kasashima S, Kawa S, Kawano M, Lauwers GY, Masaki Y, Nakanuma Y, Notohara K, Okazaki K, Ryu JK, Saeki T, Sahani DV, Smyrk TC, Stone JR, Takahira M, Webster GJ, Yamamoto M, Zamboni G, Umehara H, Stone JH (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25:1181–1192
Rosete A, Cabral AR, Kraus A, Alarcón-Segovia D (1991) Diabetes insipidus secondary to Wegener’s granulomatosis: report and review of the literature. J Rheumatol 18:761–765
Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, Rottem M, Fauci AS (1992) Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 116:488–498
Ahlström CG, Liedhölm K, Truedsson E (1953) Respirato-renal type of polyarteritis nodosa. Acta Med Scand. 144:323–332
Kapoor E, Cartin-Ceba R, Specks U, Leavitt J, Erickson B, Erickson D (2014) Pituitary dysfunction in granulomatosis with polyangiitis: the mayo clinic experience. J Clin Endocrinol Metab 99:3988–3994
Goyal M, Kucharczyk W, Keystone E (2000) Granulomatous hypophysitis due to Wegener’s granulomatosis. AJNR Am J Neuroradiol 21:1466–1469
Sampei S, Watanabe R, Ishii T, Harigae H (2014) Granulomatosis with polyangiitis preceded by central diabetes insipidus. Intern Med 53:1725–1726
Al-Fakhouri A, Manadan A, Gan J, Sreih AG (2014) Central diabetes insipidus as the presenting symptom of granulomatosis with polyangiitis. J Clin Rheumatol 20:151–154
Hughes J, Barkhoudarian G, Ciarlini P, Laws ER, Mody E, Inzucchi SE, Woodmansee WW (2013) Refractory pituitary granulomatosis with polyangiitis (Wegener’s) treated with rituximab. Endocr Pract 19:e1–e7
Pereira EA, Plaha P, Hofer M, Karavitaki N, Cudlip SA (2013) Hypophyseal Wegener’s granulomatosis presenting by visual field constriction without hypopituitarism. Clin Neurol Neurosurg 115:762–764
Slabu H, Arnason T (2013) Pituitary granulomatosis with polyangiitis. BMJ Case Rep. doi:10.1136/bcr-2013-008656
Kara O, Demirel F, Acar BC, Cakar N (2013) Wegener granulomatosis as an uncommon cause of panhypopituitarism in childhood. J Pediatr Endocrinol Metab 26:959–962
Santoro SG, Guida AH, Furioso AE, Glikman P, Rogozinski AS (2011) Panhypopituitarism due to Wegener’s granulomatosis. Arq Bras Endocrinol Metabol 55:481–485
Tenorio Jimenez C, Montalvo Valdivieso A, López Gallardo G, Mcgowan B (2011) Pituitary involvement in Wegener’s granulomatosis: unusual biochemical findings and severe malnutrition. BMJ Case Rep. doi:10.1136/bcr.02.2011.3850
Barlas NB, Hassan HH, Al Badr FB, Bilal A (2011) Structural and functional involvement of pituitary gland in Wegener’s granulomatosis. Clin Neuroradiol 21:31–33
Xue J, Wang H, Wu H, Jin Q (2009) Wegener’s granulomatosis complicated by central diabetes insipidus and peripheral neutrophy with normal pituitary in a patient. Rheumatol Int 29:1213–1217
McIntyre EA, Perros P (2007) Fatal inflammatory hypophysitis. Pituitary. 10:107–111
Thiryayi W, Donaldson MH, Border D, Tyagi A (2007) An enhancing pituitary lesion in a young woman: a diagnostic dilemma. J Clin Neurosci 14:286–288
Spísek R, Kolouchová E, Jensovský J, Rusina R, Fendrych P, Plas J, Bartůnková J (2006) Combined CNS and pituitary involvement as a primary manifestation of Wegener granulomatosis. Clin Rheumatol 25:739–742
Seror R, Mahr A, Ramanoelina J, Pagnoux C, Cohen P, Guillevin L (2006) Central nervous system involvement in Wegener granulomatosis. Medicine (Baltimore) 85:54–65
Dutta P, Hayatbhat M, Bhansali A, Bambery P, Kakar N (2006) Wegener’s granulomatosis presenting as diabetes insipidus. Exp Clin Endocrinol Diabetes 114:533–536
Düzgün N, Morris Y, Güllü S, Gürsoy A, Ensari A, Kumbasar OO, Duman M (2005) Diabetes insipidus presentation before renal and pulmonary features in a patient with Wegener’s granulomatosis. Rheumatol Int 26:80–82
Tao J, Dong Y (2003) Pituitary involvement in Wegener’s granulomatosis: a case report and review of the literature. Chin Med J (Engl) 116:1785–1788
Garovic VD, Clarke BL, Chilson TS, Specks U (2001) Diabetes insipidus and anterior pituitary insufficiency as presenting features of Wegener’s granulomatosis. Am J Kidney Dis 37:E5
Tappouni R, Burns A (2000) Pituitary involvement in Wegener’s granulomatosis. Nephrol Dial Transplant 15:2057–2058
Hajj-Ali RA, Uthman IW, Salti IA, Zaatari GS, Haddad MC, Nasr FW (1999) Wegener’s granulomatosis and diabetes insipidus. Rheumatology (Oxford) 38:684–685
Katzman GL, Langford CA, Sneller MC, Koby M, Patronas NJ (1999) Pituitary involvement by Wegener’s granulomatosis: a report of two cases. AJNR Am J Neuroradiol 20:519–523
Miesen WM, Janssens EN, van Bommel EF (1999) Diabetes insipidus as the presenting symptom of Wegener’s granulomatosis. Nephrol Dial Transplant 14:426–429
Bertken RD, Cooper VR (1997) Wegener granulomatosis causing sellar mass, hydrocephalus, and global pituitary failure. West J Med 167:44–47
Czarnecki EJ, Spickler EM (1995) MR demonstration of Wegener granulomatosis of the infundibulum, a cause of diabetes insipidus. AJNR Am J Neuroradiol 16:968–970
Roberts GA, Eren E, Sinclair H, Pelling M, Burns A, Bradford R, Maurice-Williams R, Black CM, Finer N, Bouloux PM (1995) Two cases of Wegener’s granulomatosis involving the pituitary. Clin Endocrinol (Oxf) 42:323–328
Lohr KM, Ryan LM, Toohill RJ, Anderson T (1988) Anterior pituitary involvement in Wegener’s granulomatosis. J Rheumatol 15:855–857
Hurst NP, Dunn NA, Chalmers TM (1983) Wegener’s granulomatosis complicated by diabetes insipidus. Ann Rheum Dis 42(5):600–601
Haynes BF, Fauci AS (1978) Diabetes insipidus associated with Wegener’s granulomatosis successfully treated with cyclophosphamide. N Engl J Med 299:764
Stone JH, Zen Y, Deshpande V (2012) IgG4-related disease. N Engl J Med 366:539–551
Leslie KO, Gruden JF, Parish JM, Scholand MB (2007) Transbronchial biopsy interpretation in the patient with diffuse parenchymal lung disease. Arch Pathol Lab Med 131:407–423
Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Yoshino T, Nakamura S, Kawa S, Hamano H, Kamisawa T, Shimosegawa T, Shimatsu A, Nakamura S, Ito T, Notohara K, Sumida T, Tanaka Y, Mimori T, Chiba T, Mishima M, Hibi T, Tsubouchi H, Inui K, Ohara H (2012) Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol 22:21–30
Wallace ZS, Carruthers MN, Khosroshahi A, Carruthers R, Shinagare S, Stemmer-Rachamimov A, Deshpande V, Stone JH (2013) IgG4-related disease and hypertrophic pachymeningitis. Medicine (Baltimore) 92:206–216
Schönermarck U, Lamprecht P, Csernok E, Gross WL (2001) Prevalence and spectrum of rheumatic diseases associated with proteinase 3-antineutrophil cytoplasmic antibodies (ANCA) and myeloperoxidase-ANCA. Rheumatology (Oxford) 40:178–184
Schur PH (1987) IgG subclasses—a review. Ann Allergy 58(89–96):99
Brouwer E, Tervaert JW, Horst G, Huitema MG, van der Giessen M, Limburg PC, Kallenberg CG (1991) Predominance of IgG1 and IgG4 subclasses of anti-neutrophil cytoplasmic autoantibodies (ANCA) in patients with Wegener’s granulomatosis and clinically related disorders. Clin Exp Immunol 83:379–386
Holland M, Hewins P, Goodall M, Adu D, Jefferis R, Savage CO (2004) Anti-neutrophil cytoplasm antibody IgG subclasses in Wegener’s granulomatosis: a possible pathogenic role for the IgG4 subclass. Clin Exp Immunol 138:183–192
Liu LJ, Chen M, Yu F, Zhao MH, Wang HY (2008) IgG subclass distribution, affinity of anti-myeloperoxidase antibodies in sera from patients with Wegener’s granulomatosis and microscopic polyangiitis. Nephrology (Carlton) 13:629–635
Acknowledgments
The authors are grateful to C. Ogata, K. Imura, and M. Akatsuka for their excellent technical assistance. This work was supported in part by a Grant-in-Aid for Scientific Research from the Japanese Ministry of Education, Culture, Sports, Science, and Technology 23591354, 23659477, 23591354, and 22591012, Grants-in-Aid for Scientific Research (research on hypothalamic-hypophyseal disorders) from the Ministry of Health, Labor, and Welfare, Japan.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bando, H., Iguchi, G., Fukuoka, H. et al. A diagnostic pitfall in IgG4-related hypophysitis: infiltration of IgG4-positive cells in the pituitary of granulomatosis with polyangiitis. Pituitary 18, 722–730 (2015). https://doi.org/10.1007/s11102-015-0650-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-015-0650-9