
Abstract
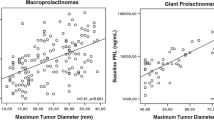
We prospectively analyzed presentations and long-term therapeutic responses to bromocriptine (BRC) in 29 newly diagnosed men with macroprolactinomas including 14 patients with 'giant prolactinoma'. Clinical symptoms, prolactin (PRL) levels and tumor size on MRI were measured before BRC and sequentially thereafter. The duration of follow-up were 6 to 96 (30.7 ± 14.4) months. Pretreatment PRL ranged between 124 and 29200 ng/mL (1698 ± 857.1) and tumor volume was between 2.81 and 132 cm3 (21.1 ± 24.3). Baseline PRL levels did not correlated with tumor volume (r = 0.45, P > 0.05). Significant decrease (P = 0.0003) in PRL, at least 96% of the pretreatment value from 1698 ± 857.1 ng/mL to 42.4 ± 30.6 ng/mL occurred in 26 patients. Persistent normalization of PRL levels (<16 ng/mL) for at least 6 months was achieved in 12 patients (40.8%). Twenty-two patients (74.8%) achieved significant tumor shrinkage (P = 0.005) at study completion. An improvement in visual field defects (VFD) and restoration of libido and potency was observed in 40% and 33.3%, respectively. Trans-sphenoidal / trans-frontal pituitary surgery was performed in 9 patients (31%) for various reasons: pituitary apoplexy in 1, CSF rhinorrhea in 2, increasing prolactin in spite of BRC therapy in 3, and intolerant /resistant to BRC in 3 patients. These data suggest that, in male macro- and giant prolactinomas, dopamine agonists represent the first-line therapy effective in reducing PRL, restoration of libido and potency, improvement of VFD and determining tumor shrinkage.
Similar content being viewed by others


Abbreviations
- BMI:
-
body mass index;
- BRC:
-
bromocriptine;
- BTHA:
-
bitemporal hemianopia;
- CSF:
-
cerebrospinal fluid;
- DA:
-
dopamine agonist;
- MRI:
-
magnetic resonance imaging;
- PRL:
-
prolactin;
- THA:
-
temporal hemianopia;
- VFD:
-
visual field defects
References
Nabarro JDN. Pituitary prolactinomas. Clin Endocrinol (Oxf) 1982;17:129–155.
Grossman A, Besser GM. Prolactinomas. BMJ 1985;290:182–184.
Colao A, Annunziato L, Lombardi G. Treatment of prolactinomas. Ann Med 1998;30:452–459.
Colao A, Di Sarno A, Cappabianca P, Briganti F, Pivonello R, Di Somma C, Faggiano A, Biondi B, Lombardi G. Gender differences in the prevalence, clinical features and response to cabergoline in hyperprolactinemia. Euro J Endocrinol 2003;148:325–331.
Colao A, Vitale G, Cappabianca P, Briganti F, Ciccarelli A, De Rosa M, Zarrilli S, Lombardi G. Outcome of cabergoline treatment in men with prolactinoma: effects of a 24-month treatment on prolactin levels, tumor mass, recovery of pituitary function, and semen analysis. J Clin Endocrinol Metab 2004;89:1704–1711.
Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R. Medical therapy of macroprolactinomas in males: I. Prevalence of hypopituitarism at diagnosis. II. Proportion of cases exhibiting recovery of pituitary function. Pituitary 2002;5:243–246.
Pinzone JJ, Katznelson L, Danila DC, Pauler DK, Miller CS, Klibanski A. Primary medical therapy of micro- and macroprolactinomas in men. J Clin Endocrinol Metab 2000;85:3053–3057.
Mindermann T, Wilson CB. Age-related and gender-related occurrence of pituitary adenomas. Clin Endocrinol (Oxf) 1994;41:359–364.
Colao A, Loche S, Cappa M, Di Sarno A, Landi ML, Sarnacchiaro F, Facciolli G, Lombardi G. Prolactinomas in children and adolescents: clinical presentation and long-term follow-up. J Clin Endocrinol Metab 1998;83:2777–2780.
Nishioka H, Haraoka J, Akada K. Growth potential of prolactinomas in men: is it really different from women? Surg Neurol 2003;59:386–390.
Calle-Rodrigue RD, Giannini C, Scheithauer BW, Lloyd RV, Wollan PC, Kovacs KT, Stefaneanu L, Ebright AB, Abboud CF, Davis DH. Prolactinomas in male and female patients: a comparative clinicopathologic study. Mayo Clin Proc 1998;73:1046–1052.
Delgrange E, Trouillas J, Maiter D, Donckier J, Tourniaire J. Sex-related difference in the growth of prolactinomas: a clinical and proliferation marker study. J Clin Endocrinol Metab 1997;82:2102–2107.
Corsello SM, Ubertini G, Altomare M, Lovicu RM, Migneco MG, Rota CA, Colosimo C. Giant prolactinomas in men: efficacy of cabergoline treatment. Clin Endocrinol (Oxf) 2003;58:662–670.
Shrivastava RK, Arginteanu MS, King WA, Post KD. Giant prolactinoma clinical management and long-term follow-up. J Neurosurg 2002;97:299–306.
Davis JRE, Sheppard MC, Heath DA. Giant invasive prolactinoma: a case report and review of nine further cases. Q J Med 1990;275:227–238.
Grote E. Characteristics of giant pituitary adenomas. Acta Neurochir 1982;60:141–153.
Majos C, Coll S, Aguilera C, Acebes JJ, Pons LC. Imaging of giant pituitary adenomas. Neuroradiology 1998;40:651–655.
Krassas GE, Pontikides N, Kaltsas T. Giant prolactinoma presented as unilateral exophthalmos in a prepubertal boy: response to cabergoline. Horm Res 1999;52:45–48.
Murphy FY, Vesely DL, Jordan RM, Flanigan S, Kohler PO. Giant invasive prolactinomas. Am J Med 1987;83:995–1002.
Grebe SKG, Delahunt JW, Feek CM. Treatment of extensive, invasive (giant) prolactinomas with bromocriptine. N Z Med J 1992;105:129–131.
Berwaerts J, Verhelst J, Abs R, Appel B, Mahler CH. Giant prolactinoma presenting with unilateral exophthalmos: effect of cabergoline and review of the literature. J Endocrinol Invest 2000;23:393–398.
Minniti G, Jaffrain-Rea ML, Santoro A, Esposito V, Ferrante L, Delfini R, Cantore G. Giant prolactinomas presenting as skull base tumors. Surg Neurol 2002;57:99–103.
Passos VQ, Souza JJ, Musolino NR, Bronstein MD. Long-term follow-up of prolactinomas: normoprolactinemia after bromocriptine withdrawal. J Clin Endocrinol Metab 2002;87:3578–3582.
Di Sarno A, Landi ML, Cappabianca P, Di Salle F, Rossi FW, Pivonello R, Di Somma C, Faggiano A, Lombardi G, Colao A. Resistance to cabergoline as compared to bromocriptine in hyperprolactinemia: prevalence, clinical definition and therapeutic strategy. J Clin Endocrinol Metab 2001;86:5256–5261.
Colao A, Di Sarno A, Landi ML, Cirillo S, Sarnacchiaro F, Facciolli G, Pivonello R, Cataldi M, Merola B, Annunziato L, Lombardi G. Long-term and low-dose treatment with cabergoline induces macroprolactinoma shrinkage. J Clin Endocrinol Metab 1997;82:3574–3579.
Colao A, Di Sarno A, Sarnacchiaro F, Ferone D, Di Renzo GF, Merola B, Annunziato L, Lombardi G. Prolactinomas resistant to standard dopamine agonists respond to chronic cabergoline treatment. J Clin Endocrinol Metab 1997;82:876–883.
Cannavò S, Curtò L, Squadrito S, Almoto B, Vieni A, Trimarchi F. A first choice treatment in patients with previously untreated prolactin-secreting pituitary adenoma. J Endocrinol Invest 1999;22:354–359.
Biller BMK, Molitch ME, Vance ML, Cannistraro KB, Davis KR, Simons JA, Schoenfelder JR, Klibanski A. Treatment of prolactin-secreting macroadenomas with the once-weekly dopamine agonist cabergoline. J Clin Endocrinol Metab 1996;81:2338–2343.
Liuzzi A, Dallabonzana D, Oppizzi G, Verde GG, Cozzi R, Chiodini P, Luccarelli G. Low doses of dopamine agonists in the long-term treatment of macroprolactinomas. N Engl J Med 1985;313:656–659.
Bevan JS, Webster J, Burke CW, Scanlon MF. Dopamine agonists and pituitary tumor shrinkage. Endocr Rev 1992;13:221–235.
Lundin P, Pedersen F. Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 1992;16:519–528.
World Health Organization (WHO). Laboratory manual for the examination of human semen and semen-cervical mucus interaction. Cambridge, UK: Cambridge University Press, 1999.
Spark RF, Willis CA, O'Reilly G, Ransil BJ, Bergland R. Hyperprolactinaemia in males with and without pituitary macroadenomas. Lancet 1982;2:129–132.
Walsh JP, Pullan PT. Hyperprolactinaemia in males: a heterogeneous disorder. Aust N Z J Med 1997;27:385–390.
Berezin M, Shimon I, Hadani M. Prolactinoma in 53 men: clinical characteristics and modes of treatment (male prolactinoma). J Endocrinol Invest 1995;18:436–441.
Hulting AL, Muhr C, Lundberg PO, Werner S. Prolactinomas in men: clinical characteristics and the effect of bromocriptine treatment. Acta Med Scand 1985;217:101–109.
Carter JN, Tyson JE, Tolis G, Van Vliet S, Faiman C, Friesen HG. Prolactin-secreting tumors and hypogonadism in 22 men. N Engl J Med 1978;299:847–852.
Creemers LB, Zelissen PMJ, van't Verlaat JW, Koppeschaar HPF. Prolactinoma and body weight: a retrospective study. Acta Endocrinol 1991;125:392–396.
Delgrange E, Donckier J, Maiter D. Hyperprolactinemia as a reversible cause of weight gain in male patients? Clin Endocrinol (Oxf) 1999;50:271–272.
Landolt AM. Cerebrospinal fluid rhinorrhoea: a complication of therapy for invasive prolactinomas. Neurosurgery 1982;11:395–401.
Leong KS, Foy PM, Swift AC, Atkin SL, Hadden DR, MacFarlane IA. CSF rhinorrhoea following treatment with dopamine agonists for massive invasive prolactinomas. Clin Endocrinol (Oxf) 2000;52:43–49.
Verhelst J, Abs R, Maiter D, van den Bruel A, Vandeweghe M, Velkeniers B, Mockel J, Lamberigts G, Petrossians P, Coremans P, Mahler C, Stevenaert A, Verlooy J, Raftopoulos C, Beckers A. Cabergoline in the treatment of hyperprolactinemia: a study in 455 patients. J Clin Endocrinol Metab 1999;84:2518–2522.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chattopadhyay, A., Bhansali, A. & Masoodi, S.R. Long-term Efficacy of Bromocriptine in Macroprolactinomas and Giant prolactinomas in Men. Pituitary 8, 147–154 (2005). https://doi.org/10.1007/s11102-005-5111-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-005-5111-4