
Abstract
Background
Gamma knife treatment outcome of large pituitary tumors which are only partially irradiated secondary to immediate proximity to critical structures such as the optic apparatus have not been rigorously studied.
Materials and methods
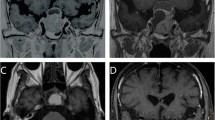
From July 2003 to December 2013, there were 41 cases of recurrent or residual nonfunctioning pituitary macroadenoma partially treated with gamma knife radiosurgery (GKRS) because the adenoma obscured part of the optic apparatus on planning SRS MR imaging.
Results
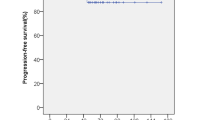
The follow up period after GKRS was 92.3 ± 5.6 months. The percentage of tumor coverage with the full dose was 88.5 ± 0.7%. Five of 43 (11.6%) patients experienced a transient visional decrease and one patient experienced a permanent visual field defect. During the follow up, two patients underwent transphenoidal surgery and one patient had a craniotomy due to tumor progression. Seven patients (16.2%) developed cortisol and thyroxine deficiencies. In multiple variant analyses, transient visual decline was correlated to the tumor volume (> 3.5 cc), percentage of tumor coverage (< 90%), the distance from the optic apparatus to the pituitary stalk (> 15 mm) and percentage of tumor above the orbital apex (65%).
Conclusion
In the limited case of this cohort, we found that partially treated pituitary nonfunctioning macroadenoma yielded a high tumor control rate. However, visual decline as a result of tumor progression or radiation effect can occur in a minority of patients. The radiosurgical technique warrants further study to better define the long-term risk to benefit profile for its use in complex pituitary macroadenoma obscuring part of the optic apparatus.




Similar content being viewed by others

Data availability
All data generated or analyzed during this study are included in this published article and its additional files.
Abbreviations
- GKRS:
-
Gamma knife radiosurgery
- Gy:
-
Gray
- MRI:
-
Magnetic resonance imaging
- PACS:
-
Picture archiving and communications system
- TOF:
-
Time of flight
- TSR:
-
Transphenoid surgery
- LH:
-
Luteinizing hormone
- FSH:
-
Follicle-stimulating hormone
- ACTH:
-
Adrenocorticotropic Hormone
- IGF-1:
-
Insulin-like growth factor 1
References
Daly AF, Rixhon M, Adam C et al (2006) High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab 91:4769–4775
Ezzat S, Asa SL, Couldwell WT et al (2004) The prevalence of pituitary adenomas: a systematic review. Cancer 101:613–619
Gondim JA, Almeida JP, Albuquerque LA et al (2014) Giant pituitary adenomas: surgical outcomes of 50 cases operated on by the endonasal endoscopic approach. World Neurosurg 82:e281–e290
Ferrante E, Ferraroni M, Castrignano T et al (2006) Non-functioning pituitary adenoma database: a useful resource to improve the clinical management of pituitary tumors. Eur J Endocrinol 155:823–829
Lucas JW, Bodach ME, Tumialan LM et al (2016) Congress of neurological surgeons systematic review and evidence-based guideline on primary management of patients with nonfunctioning pituitary adenomas. Neurosurgery 79:E533–E535
Sheehan J, Lee CC, Bodach ME et al (2016) Congress of neurological surgeons systematic review and evidence-based guideline for the management of patients with residual or recurrent nonfunctioning pituitary adenomas. Neurosurgery 79:E539–E540
Pomeraniec IJ, Kano H, Xu Z, Nguyen B et al (2017) Early versus late gamma knife radiosurgery following transsphenoidal surgery for nonfunctioning pituitary macroadenomas: a multicenter matched-cohort study. J Neurosurg. https://doi.org/10.3171/2017.5.JNS163069
Sadik ZHA, Voormolen EHJ, Depauw P et al (2017) Treatment of nonfunctional pituitary adenoma postoperative remnants: adjuvant or delayed gamma knife radiosurgery? World Neurosurg 100:361–368
Gopalan R, Schlesinger D, Vance ML et al (2011) Long-term outcomes after gamma knife radiosurgery for patients with a nonfunctioning pituitary adenoma. Neurosurgery 69:284–293
Park KJ, Kano H, Parry PV et al (2011) Long-term outcomes after gamma knife stereotactic radiosurgery for nonfunctional pituitary adenomas. Neurosurgery 69:1188–1199
Pollock BE, Cochran J, Natt N et al (2008) Gamma knife radiosurgery for patients with nonfunctioning pituitary adenomas: results from a 15-year experience. Int J Radiat Oncol Biol Phys 70:1325–1329
Sheehan JP, Starke RM, Mathieu D et al (2013) Gamma knife radiosurgery for the management of nonfunctioning pituitary adenomas: a multicenter study. J Neurosurg 119:446–456
Stafford SL, Pollock BE, Leavitt JA et al (2003) A study on the radiation tolerance of the optic nerves and chiasm after stereotactic radiosurgery. Int J Radiat Oncol Biol Phys 55:1177–1181
Cifarelli CP, Schlesinger DJ, Sheehan JP (2012) Cranial nerve dysfunction following gamma knife surgery for pituitary adenomas: long-term incidence and risk factors. J Neurosurg 116:1304–1310
Leavitt JA, Stafford SL, Link MJ et al (2013) Long-term evaluation of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Int J Radiat Oncol Biol Phys 87:524–527
Mayo C, Martel MK, Marks LB et al (2010) Radiation dose-volume effects of optic nerves and chiasm. Int J Radiat Oncol Biol Phys 76:S28-35
Pollock BE, Link MJ, Leavitt JA et al (2014) Dose-volume analysis of radiation-induced optic neuropathy after single-fraction stereotactic radiosurgery. Neurosurgery 75:456–460, discussion 460
Feigl GC, Pistracher K, Berghold A et al (2010) Pituitary insufficiency as a side effect after radiosurgery for pituitary adenomas: the role of the hypothalamus. J Neurosurg 113(Suppl):153–159
Leenstra JL, Tanaka S, Kline RW et al (2010) Factors associated with endocrine deficits after stereotactic radiosurgery of pituitary adenomas. Neurosurgery 67:27–32, discussion 32–33.
Minniti G, Osti MF, Niyazi M (2016) Target delineation and optimal radiosurgical dose for pituitary tumors. Radiat Oncol 11:135
El-Shehaby AM, Reda WA, Tawadros SR et al (2012) Low-dose gamma knife surgery for nonfunctioning pituitary adenomas. J Neurosurg 117(Suppl):84–88
Kim M, Paeng S, Pyo S et al (2006) Gamma knife surgery for invasive pituitary macroadenoma. J Neurosurg 105(Suppl):26–30
Mingione V, Yen CP, Vance ML et al (2006) Gamma surgery in the treatment of nonsecretory pituitary macroadenoma. J Neurosurg 104:876–883
Starke RM, Williams BJ, Jane JA et al (2012) Gamma knife surgery for patients with nonfunctioning pituitary macroadenomas: predictors of tumor control, neurological deficits, and hypopituitarism. J Neurosurg 117:129–135
Pan HC, Cheng FC, Sun MH et al (2007) Prediction of volumetric data errors in patients treated with gamma knife radiosurgery. Stereotact Funct Neurosurg 85:184–191
Pan HC, Sun MH, Chen CC et al (2008) Neuroimaging and quality-of-life outcomes in patients with brain metastasis and peritumoral edema who undergo gamma knife surgery. J Neurosurg 109(Suppl):90–98
Kondziolka D, Shin SM, Brunswick A et al (2015) The biology of radiosurgery and its clinical applications for brain tumors. Neuro Oncol 17:29–44
Mortini P, Barzaghi R, Losa M et al (2007) Surgical treatment of giant pituitary adenomas: strategies and results in a series of 95 consecutive patients. Neurosurgery 60:993–1002, discussion 1003–1004.
Sebastian P, Balakrishnan R, Yadav B et al (2016) Outcome of radiotherapy for pituitary adenomas. Rep Pract Oncol Radiother 21:466–472
Zhao K, Liu X, Liu D et al (2016) Fractionated gamma knife surgery for giant pituitary adenomas. Clin Neurol Neurosurg 150:139–142
Minniti G, Scaringi C, Poggi M et al (2015) Fractionated stereotactic radiotherapy for large and invasive non-functioning pituitary adenomas: long-term clinical outcomes and volumetric MRI assessment of tumor response. Eur J Endocrinol 172:433–441
Acknowledgements
The authors would like to thanks all assistant and Biostatistics Task Force of Taichung Veterans General Hospital for their kind assistances in the manuscript preparation and statistical analysis.
Funding
The funding (TCVGH-1064903C and TCVGH-PU1068101) was received from Taichung Veterans General Hospital, Taichung, Taiwan.
Author information
Authors and Affiliations
Contributions
SCC and YMC collected the data and wrote the manuscript. SMH, LSD and THK collected the data of imaging and visual field for analysis. CYJ and SML helped in statistical analysis. SJ helped to design this study. PHC conducted the study design and collected the data and edited the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There was no conflict of interest.
Ethical approval
Approval by ethical committee of Taichung Veterans General Hospital is on record No. CG12718B.
Rights and permissions
About this article

Cite this article
Shen, CC., You, WC., Sun, MH. et al. Outcome of partially irradiated recurrent nonfunctioning pituitary macroadenoma by gamma knife radiosurgery. J Neurooncol 139, 767–775 (2018). https://doi.org/10.1007/s11060-018-2925-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-018-2925-2