
Abstract
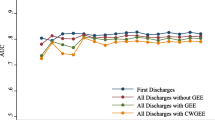
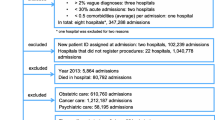
The use of hierarchical logistic regression for provider profiling has been recommended due to the clustering of patients within hospitals, but has some associated difficulties. We assess changes in hospital outlier status based on standard logistic versus hierarchical logistic modelling of mortality. The study population consisted of all patients admitted to acute, non-specialist hospitals in England between 2007 and 2011 with a primary diagnosis of acute myocardial infarction, acute cerebrovascular disease or fracture of neck of femur or a primary procedure of coronary artery bypass graft or repair of abdominal aortic aneurysm. We compared standardised mortality ratios (SMRs) from non-hierarchical models with SMRs from hierarchical models, without and with shrinkage estimates of the predicted probabilities (Model 1 and Model 2). The SMRs from standard logistic and hierarchical models were highly statistically significantly correlated (r > 0.91, p = 0.01). More outliers were recorded in the standard logistic regression than hierarchical modelling only when using shrinkage estimates (Model 2): 21 hospitals (out of a cumulative number of 565 pairs of hospitals under study) changed from a low outlier and 8 hospitals changed from a high outlier based on the logistic regression to a not-an-outlier based on shrinkage estimates. Both standard logistic and hierarchical modelling have identified nearly the same hospitals as mortality outliers. The choice of methodological approach should, however, also consider whether the modelling aim is judgment or improvement, as shrinkage may be more appropriate for the former than the latter.
Similar content being viewed by others

References
Jarman, B., Gault, S., Alves, B., et al., Explaining differences in English hospital death rates using routinely collected data. BMJ 318:1515–1520, 1999.
Aylin, P., Bottle, A., Jen, M. H., et al., HSMR mortality indicators. http://www1.imperial.ac.uk/resources/3321CA24-A5BC-4A91-9CC9-12C74AA72FDC Accessed 10 May 2013.
Bottle, A., and Aylin, P., Intelligent information: A national system for monitoring clinical performance. Health Serv. Res. 43:10–31, 2008.
Alharbi, O., Rabeneck, L., Paszat, L. F., et al., A population-based analysis of outpatient colonoscopy in adults assisted by an anaesthesiologist. Anaesthesiology 111:734–740, 2009.
Krumholz, H. M., Brindis, R. G., Brush, J. E., et al., Standards for statistical models used for public reporting of health outcomes. Circulation 113:456–462, 2006.
Cohen, L. H., Cardiac surgery in the adult. 3rd edition. http://cardiacsurgery.ctsnetbooks.org/ Accessed 20 March 2013.
DeLong, E., Hierarchical modeling: Its time has come. Am. Heart J. 145:16–18, 2003.
Diez-Roux, A. V., Multilevel analysis in public health research. Annu. Rev. Public Health 21:171–192, 2000.
Steele, F., Module 5: Introduction to multilevel modelling concepts. http://www.cmm.bristol.ac.uk/learning-training/ Accessed 1 August 2013.
Hox, J. J., Applied multilevel analysis. TT Publikaties Amsterdam, 1995. http://www.eric.ed.gov/PDFS/ED384636.pdf Accessed 1 August 2013.
Alexandrescu, R., Jen, M. H., Bottle, A., et al., Logistic vs. Hierarchical modeling: An analysis of a statewide inpatient sample. J. Am. Coll. Surg. 213:392–401, 2011.
The Information centre. Hospital episode statistics. 2011. www.hesonline.nhs.uk/ Accessed 11 March 2013.
NHS Connecting for Health. Secondary users service. 2011. http://www.connectingforhealth.nhs.uk/systemsandservices/sus Accessed 11 March 2013.
HCUP CCS: Healthcare Cost and Utilization Project (HCUP). Clinical Classifications Software (CCS) for ICD-10. Agency for Healthcare and Quality, Rockville, MD 2009. http://www.hcup-us.ahrq.gov/toolssoftware/icd_10/ccs_icd_10.jsp Accessed 11 March 2013.
Sundararajan, V., Henderson, T., Perry, C., et al., New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 57:1288–1294, 2004.
Gridlink. Office for National Statistics. 2011. http://www.ons.gov.uk/ons/guide-method/geography/geographic-policy/gridlink-/index.html.
Wong, S., Flowers, J., and Lyratzopoulos, Y., Hospital admissions for myocardial infarction in the East of England, 1997/98–2007/08. Available from: http://www.erpho.org.uk/Download/Public/18587/1/Briefing%2020%20STEMI%204%20sides%20A4%20FINAL.pdf Accessed 1 August 2013.
Seccareccia, F., Perucci, C. A., D’Errigo, P., et al., The Italian CABG Outcome Study: Short-term outcomes in patients with coronary artery bypass graft surgery. Eur. J. Cardiothorac. Surg. 29:56–62, 2006.
Grant, S. W., Grayson, A. D., Purkayastha, D., et al., Logistic risk model for mortality following elective abdominal aortic aneurysm repair. Br. J. Surg. 98:652–658, 2011.
SAS Institute Inc, SAS/STAT® 9.2 user’s guide. The GLIMMIX procedure. SAS Institute Inc., Cary, NC, 2008.
Cohen, M. E., Dimick, J. B., Bilimoria, K. Y., et al., Risk adjustment in the American College of Surgeons National Surgical Quality Improvement Program: A comparison of logistic versus hierarchical modeling. J. Am. Coll. Surg. 209:687–693, 2009.
Cohen, M. E., Ko, C. Y., Bilimoria, K. Y., et al., Optimizing ACS NSQIP modeling for evaluation of surgical quality and risk: Patient risk adjustment, procedure mix adjustment, shrinkage adjustment, and surgical focus. J. Am. Coll. Surg. 217:336–346, 2013.
Glance, L. G., Dick, A., Osler, T. M., et al., Impact of changing the statistical methodology on hospital and surgeon ranking: The case of the New York State cardiac surgery report card. Med. Care 44:311–319, 2006.
The Centre for Medicare and Medicaid Services. Statistical issues in assessing hospital performance. http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Downloads/Statistical-Issues-in-Assessing-Hospital-Performance.pdf Accessed 1 August 2013.
Spiegelhalter, D. J., Funnel plots for comparing institutional performance. Stat. Med. 24:1185–1202, 2005.
Cook, N. R., Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation 115:928–935, 2007.
Snijders, T. A. B., and Bosker, R. J., Multilevel analysis. An introduction to basic and advanced multilevel modeling. SAGE Publications, London, 1999.
D’Errigo, P., Tosti, M. E., Fusco, D., et al., Use of hierarchical models to evaluate performance of cardiac surgery centres in the Italian CABG outcome study. BMC Med. Res. Methodol. 7:29, 2007.
Hannan, E. L., Wu, C., DeLong, E. R., and Raudenbush, S. W., Predicting risk-adjusted mortality for CABG surgery: Logistic versus hierarchical logistic models. Med. Care 43:726–735, 2005.
Austin, P. C., Alter, D. A., and Tu, J. V., The use of fixed- and random-effects models for classifying hospitals as mortality outliers: A Monte Carlo assessment. Med. Decis. Making 23:526–539, 2003.
Austin, P. C., Tu, J. V., and Alter, D. A., Comparing hierarchical modeling with traditional logistic regression analysis among patients hospitalized with acute myocardial infarction: Should we be analyzing cardiovascular outcomes data differently? Am. Heart J. 145:27–35, 2003.
Clark, D. E., Hannan, E. L., and Wu, C., Predicting risk adjusted mortality for trauma patients: Logistic versus multilevel logistic models. J. Am. Coll. Surg. 211:224–231, 2010.
Tan, A., Freeman, J. L., and Freeman, D. H., Jr., Evaluating health care performance: Strengths and limitations of multilevel analysis. Biom. J. 49:707–718, 2007.
Mohammed, M. A., Manktelow, B. N., and Hofer, T. P., Comparison of four methods for deriving hospital standardised mortality ratios from a single hierarchical logistic regression model. Stat. Methods Med. Res. Nov 6, 2012.
Bland, J. M., and Altman, D. G., Measuring agreement in method comparison studies. Stat. Methods Med. Res. 8:135–160, 1999.
Acknowledgments
The Dr Foster Unit is largely funded by a research grant from Dr Foster Intelligence, an independent healthcare information company and joint venture with the UK Department of Health. The Dr Foster Unit at Imperial is affiliated with the Centre for Patient Safety and Service Quality at Imperial College Healthcare NHS Trust and funded by the National Institute of Health Research. We are grateful for support from the NIHR Biomedical Research Centre funding scheme.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics
We have permission from the NIGB under Section 251 of the NHS Act 2006 (formerly Section 60 approval from the Patient Information Advisory Group) to hold confidential data and analyse them for research purposes. We have approval to use them for research and measuring quality of delivery of healthcare, from the South East Ethics Research Committee.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Systems-Level Quality Improvement
Rights and permissions
About this article
Cite this article
Alexandrescu, R., Bottle, A., Jarman, B. et al. Classifying Hospitals as Mortality Outliers: Logistic Versus Hierarchical Logistic Models. J Med Syst 38, 29 (2014). https://doi.org/10.1007/s10916-014-0029-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-014-0029-x