
Abstract
Genetic counselors experience high rates of compassion fatigue and an elevated risk for burnout, both of which can negatively impact patient care and retention in the profession. In other healthcare professions, mindfulness training has been successfully used to address similar negative psychological sequelae and to bolster empathy, which is the foundation of our counseling work. We aimed to assess associations between mindfulness and key professional variables, including burnout, compassion fatigue, work engagement, and empathy. Data were collected via an anonymous, online survey that included validated measures of mindfulness and these key professional variables. The survey was completed by 441 genetic counselors involved in direct patient care. Half of the respondents (50.1%) reported engaging in yoga, meditation, and/or breathing exercises. Mindfulness was positively correlated with work engagement (r = 0.24, p < 0.001) and empathy (as measured through four subscales: perspective taking (r = 0.15, p = 0.002), empathic concern (r = 0.11, p = 0.03), fantasy (r = − 0.11, p = 0.03) and personal distress (r = − 0.15, p = 0.001)). Mindfulness was negatively correlated with compassion fatigue (r = − 0.48, p < 0.001) and burnout (r = − 0.50, p < 0.001). Given these findings, mindfulness training may be a valuable addition to graduate and continuing education for genetic counselors. The integration of mindfulness into the genetic counseling field will likely improve professional morale and well-being, while promoting workforce retention and bolstering the relational and counseling aspects of our clinical work.
Similar content being viewed by others


Introduction
Like many helping professionals, genetic counselors need to sustain compassion and empathy while repeatedly experiencing the distress of their clients. It has previously been documented that among genetics professionals, genetic counselors are particularly at risk for high rates of distress and burnout, as well as reduced professional satisfaction (Bernhardt et al. 2009). More recently, pressures on genetic counselors have been building as need for our services and caseloads increase (Pan et al. 2016). Given these demands, the profession would benefit from interventions that address burnout and compassion fatigue while sustaining empathy and compassion.
In multiple studies, genetic counselors have been found to be at risk for burnout (Bernhardt et al. 2009) and compassion fatigue (Benoit et al. 2007; Lee et al. 2015; Injeyan et al. 2011; Udipi et al. 2008). Across a range of healthcare professions, these psychological sequelae have been found to negatively impact retention in the profession (Coomber and Louise Barriball 2007; Hayes et al. 2006; Van Bogaert et al. 2013) and quality of patient care (Bernhardt et al. 2009; Cohen-Katz et al. 2005; Duchemin et al. 2015; Grepmair et al. 2007; Haas et al. 2000; Hu et al. 2012; Kearney et al. 2009; Krasner et al. 2009; Shanafelt et al. 2002; Shapiro et al. 2007). Up to 32% of genetic service providers have been found to experience at least moderate levels of distress, which is a significant risk factor for burnout (Bernhardt et al. 2009; Geller et al. 2010). An individual suffering from burnout typically experiences professional dissatisfaction by losing enthusiasm for work and no longer finding meaning in his or her profession (Shanafelt 2009). Specifically, for healthcare providers, burnout has been negatively associated with personal health, job performance, productivity, professionalism, empathy, and compassion (Shanafelt 2009; Zwack and Schweitzer 2013). Minimizing burnout in the profession is valuable not only because of the impact on the quality of life of individual genetic counselors, but also because burnout leads people to leave helping professions (Bernhardt et al. 2009; Geller et al. 2010; Krasner et al. 2009). This consequence is especially concerning for genetic counselors because the demand for our services is growing rapidly, making retention increasingly critical (Pan et al. 2016).
While burnout has implications for genetic counselors’ professional satisfaction and retention, it is also important to consider how distress can impact genetic counselors’ personal well-being and ability to provide high quality services to patients. Distress can lead to a state of feeling overwhelmed by constantly experiencing patients’ suffering, or compassion fatigue (Udipi et al. 2008). Up to three-quarters of genetic counselors are found to be at moderate to high risk for compassion fatigue (Injeyan et al. 2011; Lee et al. 2015; Udipi et al. 2008). Compassion fatigue can impede patient care, as counselors tend to disengage from their patients to protect their emotional state (Udipi et al. 2008). In contrast, empathy has positive effects on quality of patient care and is an integral component of the counselor-patient relationship (Veach et al. 2003). Empathy involves understanding the patient’s lived reality—his or her past or present experiences, emotions, and perceptions—and identifying how it impacts their behavior (Weil 2000). The literature suggests that this deep connection impacts quality of patient care by facilitating enhanced coping, treatment adherence, trust, and willingness to disclose fuller medical histories (Halpern 2003). Given these implications, it would be advantageous to find strategies to increase genetic counselors’ ability to engage in empathic understanding, while also defending against the high risk of compassion fatigue.
When considering how other professions have bolstered empathy and mitigated burnout and compassion fatigue, mindfulness training comes to the forefront of the literature. Mindfulness is considered “a state of mind in which one is highly aware and focused on the reality of the present moment, accepting and acknowledging it, without getting caught up in the thoughts that are about the situation or emotional reactions to the situation” (p. 71, Bishop 2002). It has been suggested that clinicians can learn four specific habits of mindfulness through mindfulness training: (1) attentive observation of oneself, the patient and the patient’s problem, (2) critical curiosity and courage to recognize one’s weaknesses, ((3) a toleration of uncertainty and ability to allow preconceived ideas to pass, and (4) focused presence and compassion, resulting in a valuable patient-clinician connection (Epstein 1999).
Multiple intervention studies have demonstrated a myriad of both personal and professional benefits as a result of mindfulness training (see Lamothe et al. 2015 for systematic review of mindfulness training for healthcare professionals). Mindfulness training among healthcare providers has been found to lead to decreased stress, anxiety, burnout, emotional exhaustion, and depersonalization, while also increasing work engagement, empathy, sense of well-being and personal accomplishment, self-awareness, and the ability to understand the connection between emotions and behavior (Bernhardt et al. 2010; Cohen-Katz et al. 2005; Dobie 2007; Goodman and Schorling 2012; Krasner et al. 2009; Lamothe et al. 2015). Positive outcomes from mindfulness training have been observed in a wide range of clinical professions including nurses, mental health professionals, physicians, oncologists, social workers, and physical therapists. Additionally, mindfulness training may represent “preventative treatment” for the subset of clinical trainees who are at particularly high risk for burnout and compassion fatigue (Shapiro et al. 2007). While mindfulness has been studied in a myriad of healthcare professions, it has not been examined in the genetic counseling profession.
Hypotheses
Given the positive impact of mindfulness seen in other healthcare professions, we hypothesized that mindfulness among genetic counselors could influence key factors that have the potential to impact professional satisfaction and retention, as well as the quality of patient care (Fig. 1). Specifically, we hypothesized that mindfulness is positively associated with empathy and work engagement and negatively associated with burnout and compassion fatigue (Fig. 1). Additionally, we sought to describe participation in mindfulness activities among genetic counselors and hypothesized that participation would be positively associated with mindfulness.

Proposed framework for leveraging mindfulness as a method to promote retention and quality of care in the genetic counseling profession. A graphical representation of the hypothesized relationships between the main study variables. Upward arrows indicate a positive association between variables, while downward arrows indicate a negative association
Methods
Study Design
We performed a cross-sectional, quantitative study of currently practicing genetic counselors who provide direct clinical care to patients.
Stanford University’s institutional review board approved this study.
Recruitment
An invitation to participate was emailed in October 2016 through the National Society of Genetic Counselors (NSGC) Student Research Survey Program (N~3500), with a reminder email 3 weeks later. In order to minimize response bias, the email described the study as investigating factors that have the potential to impact professional satisfaction and quality of patient care, and specifically did not mention mindfulness. Informed consent was obtained from all participants. Our study included the following inclusion criteria: (1) respondents must be currently practicing genetic counselors and (2) respondents must provide direct clinical care to patients.
Instrumentation
Data were collected using an anonymous online survey. The survey included the four standardized measures reviewed below. The survey also included questions on respondents’ demographics, participation in mindfulness activities, and interest in participating in future research on this topic. Participation in mindfulness activities was asked as a series of yes/no questions for meditation, yoga, and breathing exercises.
Independent Variable
Mindfulness
The Mindfulness Attention Awareness Scale (MAAS; Brown and Ryan 2003) is a 15-item instrument that has been used widely in the mindfulness literature. The MAAS has good internal consistency (Cronbach’s alpha 0.79) and uses a 6-point Likert scale (1 = almost always, 6 = almost never) (Brown and Ryan 2003). This measure specifically assesses an individual’s ability to be openly attentive to, and aware of, present events and experiences by focusing on both internal states and overt behaviors. Scoring involves averaging the respondents’ responses, which produces a total mindfulness score between 1 and 6. Higher scores represent greater mindfulness levels.
Dependent Variables
Empathy
Empathy is understood to be a multidimensional construct (Davis 1980). The Interpersonal Reactivity Index (IRI; Davis 1980) is a widely used and validated 28-item measure comprised of four separate subscales that each assess a separate aspect of the global concept of empathy. The IRI has been used to measure self-reported levels of empathy among a variety of healthcare providers and trainees, including nurses, nursing students, medical students, and physicians (Beddoe and Murphy 2004; Beckman et al. 2012; Costa et al. 2017; Kesbakhi et al. 2017). Each subscale is measured using a 5-point Likert scale (1 = does not describe me well, 5 = describes me very well), has good Cronbach’s alpha scores (0.73–0.79), and has adequate test-retest reliability (r = 0.61–0.81).
The perspective-taking scale measures one’s ability to adopt the perspective of other people by taking their point of view. The empathic concern scale measures qualities of warmth, compassion, and concern for others. The fantasy subscale measures an individual’s tendencies to identify with characters in fictional situations. Lastly, the personal distress scale measures discomfort and anxiety that result from observing another’s negative experience. The fantasy and personal distress subscales are inversely related to empathy; those who score high on the fantasy scale show greater psychological arousal and those who have higher personal distress scores show greater discomfort in emotional social settings (Davis 1983). The subscales are not scored cumulatively; high scores in the perspective taking and empathic concern subscales and low scores in the fantasy and personal distress subscales represent higher global empathy.
Burnout and Compassion Fatigue
The Professional Quality of Life scale (ProQOL; Stamm 2010) has been used with good construct validity in over 200 studies (Stamm 2010). The ProQOL 5 is a 30-item measure that assesses positive and negative effects of working with distressed people through three subscales: burnout, secondary traumatic stress, and compassion satisfaction (Cronbach’s alpha scores of 0.75–0.88; Stamm 2010). Burnout was measured using the burnout subscale, which measures a person’s feelings of hopelessness and despair due to difficulties at work and the perception that work-related efforts are ineffective (Stamm 2010). Compassion fatigue was measured using the secondary traumatic stress subscale (previously labeled the compassion fatigue subscale in earlier versions of the ProQOL), which assesses effects of second-hand exposure to stressful events, such as being empathically engaged in other’s emotional distress (Stamm 2010). The compassion satisfaction subscale was not used for analyses in this study; however, to maintain internal reliability, the subscale was still included in our survey. Each subscale is comprised of 10 statements, rated on a five-point Likert scale (1 = never, 5 = very often). Higher scores on each subscale indicate a higher level of the construct being assessed.
Of note, two prior studies that used the ProQOL with genetic counselors modified five items to better reflect the nature of genetic counseling clinical experiences (Lee et al. 2015; Udipi et al. 2008). These authors noted no significant changes to the internal reliability of the measure; thus, these amendments were used in this study.
Work Engagement
The Utrecht Work Engagement Scale (UWES; Schaufeli and Bakker 2003) is a 17-item measure that assesses work engagement with high internal consistency (Cronbach’s alpha scores of 0.91–0.96) and adequate test-retest reliability (r = 0.63–0.72). The UWES has been validated and translated in over 10 different languages and has been used in research worldwide among different occupational groups (Schaufeli and Bakker 2003). Of note, the UWES has been used in recent literature to measure work engagement among intensive care professionals, physicians, and hospital nurses (Kunie et al. 2017; Loerbroks et al. 2017; Van Mol et al. 2017). The UWES is comprised of three subscales: vigor, dedication, and absorption. High levels of energy, resilience, and persistence characterize having vigor in one’s work environment (Schaufeli and Bakker 2003). Dedication refers to being strongly committed to one’s work by demonstrating pride, sense of purpose, and enthusiasm (Schaufeli and Bakker 2003). Lastly, absorption demonstrates being fully engaged and happily consumed by one’s work (Schaufeli and Bakker 2003). Each subscale is comprised of 5 to 6 statements, which are assessed using a 7-point Likert scale (0 = never, 6 = always). Scoring permits a total work engagement score for each respondent (between 0 and 6), with higher scores signifying greater work engagement.
Data Analysis
Survey responses were recorded using Qualtrics and statistical analyses were performed in SPSS (version 24.0). The scores on the mindfulness scale followed a normal distribution; however, the dependent variable scores strayed slightly from normality. Therefore, Spearman’s Rho, a non-parametric measure of correlation, was utilized to assess correlations between mindfulness and the dependent variables. Independent t tests and ANOVA were used to compare these mindfulness scores and subscale scores between those who reported participating in mindfulness activities and those who did not. Significance levels are reported as 2-tailed p values, with an alpha of 0.05 used as a cutoff for statistical significance.
Results
Respondent Characteristics
A total of 441 genetic counselors completed the survey (a conservatively estimated response rate of 12.6%). Most respondents were female (97.5%), identified as Caucasian (92.7%) and their mean age was 33.9 years (SD = 9.3, range = 23–68) (Table 1). A majority of respondents worked full time (90.2%). These demographics are consistent with the profession overall (Professional Status Survey, NSGC 2016).
Mean scores for key measures are displayed in Table 2 and compared to published means for general population samples and healthcare provider samples in Table SII. Genetic counselors had higher scores of mindfulness and empathy than general population samples but comparable scores to other clinicians (Table SII). On burnout and compassion fatigue, genetic counselors scored higher than pooled samples but similar to other clinicians (Table SII). Work engagement was higher in our sample than in other working professionals or physicians (Table SII).
We asked whether participants take part in yoga, meditation, and/or breathing exercises to gain a sense of the current practice of what are typically thought of as mindfulness activities. Half of participants (50.1%) reported engaging in at least one of these activities (yoga 34.7%, meditation 14.5%, breathing exercises 30.8%) (Table 1; Table SI). There was no significant difference in mindfulness scores among those who engage in yoga (p = 0.25), meditation (p = 0.16), breathing exercises (p = 0.07), or any of these three activities (p = 0.38) versus those who do not (Table SI).
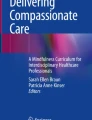
There was a significant but weak correlation between empathy and mindfulness, as indicated by positive correlations with the perspective taking (r = 0.145, p = 0.002) and empathic concern subscales of the IRI (r = 0.107, p = 0.03), and negative correlations with the fantasy (r = − 0.103, p = 0.03) and personal distress subscales (r = − 0.151, p = 0.001) of the IRI (Table 2, Fig. 2). Mindfulness was also positively associated with work engagement (UWES; r = 0.237, p < .001) (Table 2, Fig. 2). We observed moderate negative associations between mindfulness and compassion fatigue (ProQOL5 subscale; r = − 0.480, p < 0.001), as well as burnout (ProQOL5 subscale; r = − 0.503, p < 0.001) (Table 2, Fig. 2).

Correlations between mindfulness and outcome variables in the present study. A graphical representation of the correlations between mindfulness and outcomes. Upward arrows indicate a positive correlation between the two variables, while downward arrows indicate a negative correlation between the two variables. Correlation coefficients (r) and significance (p values) are provided. 1Not significant
Discussion
Our study demonstrates that mindfulness among genetic counselors has beneficial associations with key professional outcomes, including burnout, compassion fatigue, work engagement, and empathy. Prior literature suggests that these variables have the potential to affect professional satisfaction, (Bernhardt et al. 2009; Epstein 1999; Kearney et al. 2009; Krasner et al. 2009; Lee et al. 2015; Shanafelt 2009; Van Bogaert et al. 2013), retention (Coomber and Louise Barriball 2007; Okie 2008; Hayes et al. 2006; Williams et al. 2010; Van Bogaert et al. 2013) and quality of patient care (Bernhardt et al. 2009; Cohen-Katz et al. 2005; Duchemin et al. 2015; Grepmair et al. 2007; Haas et al. 2000; Hu et al. 2012; Kearney et al. 2009; Krasner et al. 2009; Shanafelt et al. 2002; Shapiro et al. 2007) (Fig. 1). Given these positive implications for providers, trainees, and patients, there has been widespread inclusion of mindfulness training in healthcare education systems in a variety of hospital and clinical training settings (Ruff and Mackenzie 2009). Our findings suggest that a similar integration of mindfulness training into the graduate and continuing education of genetic counselors would benefit genetic counselors and their patients.
A Pathway to Improved Genetic Counselor Professional Well-Being and Retention
There is a need to decrease the high rates of burnout and compassion fatigue among genetic counselors in order to bolster well-being and maximize retention. Currently, the demand for genetic counselors exceeds the supply, suggesting the profession needs to be strategic to ensure retention and address workforce issues (Pan et al. 2016). Moreover, retention has implications for patient access. Increasing mindfulness might bolster retention and thus help maximize the size of the genetic counseling workforce, which in turn would help enhance patient access. Of note, when considering retention in our field at large, 42.4% of clinical genetic counselors who have left or thought about leaving the profession, cite burnout and compassion fatigue as major reasons (NSGC 2016).
Our data, combined with the findings of prior studies, suggest that mindfulness might improve professional well-being and retention via increased work engagement and decreased burnout and compassion fatigue (Fig. 2). Work engagement is characterized by a heightened energetic, passionate connection with work and an ability to handle the demands of a profession (Schaufeli et al. 2006). Achieving professional engagement can lead to job satisfaction through a sense of competence, pleasure and control over work, which defends against the symptoms of burnout (Schaufeli and Bakker 2003). It is evident in the literature on other healthcare providers that high rates of work engagement or job satisfaction and low rates of burnout are associated with decreased turnover (Coomber and Louise Barriball 2007; Okie 2008; Hayes et al. 2006; Van Bogaert et al. 2013). Compassion fatigue among genetic counselors also poses a potential threat to the stability of our workforce. Counseling becomes less meaningful and satisfying when one experiences compassion fatigue, as counselors typically disengage from empathic understanding (Udipi et al. 2008); often individuals cite feelings of guilt and regret about their diminished role in the counseling process (Udipi et al. 2008). These isolating emotions result in decreased professional satisfaction and can also stimulate thoughts of leaving the profession.
It appears that increasing work engagement while simultaneously decreasing burnout and compassion fatigue would improve professional satisfaction, morale, and workforce stability. The importance of workforce issues is demonstrated by the fact that one of the main goals outlined in the current National Society of Genetic Counselors (NSGC) Strategic Plan, is to “direct the evolution and adaptation of the genetic counselor workforce” (April 10, 2017, p. 1). Our findings, in addition to previous literature, suggest mindfulness has positive implications with regard to these specific variables (Beddoe and Murphy 2004; Bernhardt et al. 2010; Kearney et al. 2009; Udipi et al. 2008; Van Bogaert et al. 2013) (Fig. 2). Mindfulness training could be a unique and efficacious tool that could address workforce issues by promoting professional satisfaction and increased retention among genetic counselors (Fig. 1).
A Pathway to Improved Clinical Care
Our data suggest that increased mindfulness among genetic counselors could be used to improve the quality of clinical care and patient outcomes, via increased empathy, decreased burnout, and decreased compassion fatigue (Fig. 2).
Compassion fatigue, often described as “the cost of caring” (Kearney et al. 2009), has a negative impact on clinical care. To counteract the overwhelming absorption of patient emotions that is experienced through compassion fatigue, providers tend to distance themselves from their patients and refrain from engaging in empathic understanding (Udipi et al. 2008). This detachment negatively impacts the quality of patient care and may lead to reductions in patients’ confidence, perceived support, and trust in the counselor-patient relationship (Connelly 1999).
In contrast, empathy is widely accepted as an integral aspect of genetic counselor efficacy and the foundation of the relational and psychological aspects of our work. Empathy involves three components: (1) affective awareness, wherein the genetic counselor can perceive the meaning and feelings of another, (2) cognitive reasoning, which involves taking the patient’s perspective to understand his/her frame of reference, and (3) communication, where a genetic counselor reflects and clarifies the patient’s feelings to provide meaning to their situation (Wiseman 1996). Carl Rogers, the father of Person-Centered therapy, stressed that a counselor’s ability to be empathic is necessary for clients to be able to make meaningful change (Caldwell 2012). Therefore, empathy became the backbone of Rogerian counseling theory (Davis 1990), which in turn formed the foundation of genetic counseling. Similarly, the “Reciprocal-Engagement Model” (REM), a model for genetic counseling practice, highlights the counselor-client relationship as integral to the genetic counseling process (Veach et al. 2007). REM recognizes that outcomes of a genetic counseling session are dependent on the quality of connection established between the counselor and patient (Veach et al. 2007). Specifically, an emphasis on psychological dimensions of practice within genetic counseling sessions, such as using empathic responses, is associated with positive client outcomes (Meiser et al. 2008).
Given these considerations, enhanced empathy and reduced compassion fatigue would be expected to improve the quality of patient care in genetic counseling. Our findings and prior literature point to mindfulness as a potential tool to support and enhance the relational and psychological aspects of our work with patients (Beddoe and Murphy 2004; Krasner et al. 2009; Shanafelt et al. 2002; Shapiro et al. 1998). Consistent with this, a randomized controlled trial of meditation in psychotherapists in training found patient outcomes were improved when the psychotherapist meditated (Grepmair et al. 2007).
While we observed a significant correlation between mindfulness and empathy, the correlation was weak, which raises the question of how impactful mindfulness training would be on genetic counselor empathy. Prior research on mindfulness and empathy in other clinicians provide some insight. The relationship between mindfulness and empathy is robust, having been observed in multiple studies (Asuero et al. 2014; Barbosa et al. 2013; Bazarko et al. 2013, Birnie et al. 2010; Beddoe and Murphy 2004; Cohen-Katz et al. 2005; Krasner et al. 2009; Shapiro et al. 1998). The effect sizes of mindfulness interventions to increase empathy (0.34 to 0.71, (Asuero et al. 2014; Birnie et al. 2010; Krasner et al. 2009; Lamothe et al. 2018)) are comparable to effect sizes of other interventions aimed at increasing clinician empathy (mean 0.80 (95% CI 0.4–1.20)), albeit perhaps on the lower end of that range (Kiosses et al. 2016). This suggests that mindfulness training is likely to improve counselor empathy, though it may not be the most potent empathy-enhancing intervention. It is also possible that the correlation between mindfulness and empathy in our study was small because of a ceiling effect.
Interestingly empathy can also be a liability, if not established with self-awareness and effective boundaries. Repeated empathic engagements with distressed patients can result in compassion fatigue (Udipi et al. 2008). However, our study demonstrates that mindfulness among genetic counselors is significantly associated with both lower levels of compassion fatigue and higher levels of empathy. This suggests that mindfulness may play a role in strengthening empathy while protecting counselors from compassion fatigue. The term “exquisite empathy,” has been proposed in the literature to distinguish a form of empathy that is highly present and performed with healthy boundaries (Kearney et al. 2009). This form of empathy decreases the emotional depletion that presents in compassion fatigue and facilitates the nourishing heartfelt empathic engagement that invigorates the patient-counselor relationship (Kearney et al. 2009). It is possible that the self-awareness attained through mindfulness uniquely fosters this form of empathy and thus explains the positive correlation with empathy, despite a negative correlation with compassion fatigue.
Mindfulness Training
The majority of research on the development and outcomes of mindfulness focus on a specific training program created by Dr. Jon Kabat-Zinn, called mindfulness-based stress reduction (MBSR), which follows a defined protocol and curriculum. The traditional MBSR training consists of an 8-week course that meets weekly for 2.5 hours and for a single all-day training (Kabat-Zinn 1994; Santorelli et al. 2017; Stahl and Goldstein 2010). Participants are trained on a range of formal meditation practices including mindfulness of the breath, body, movement, and thoughts. In addition to in-class training, MBSR involves daily homework in which participants practice different forms of mindfulness activities on their own, often with the support of an audio-recording provided by their teacher. Within the healthcare setting, MBSR has been seen to improve both psychological and physical outcomes among patients with a myriad of mental and physical illnesses (see Gotink et al. 2015 systematic review and meta-analysis). Among healthcare providers, MBSR has led to improvements in burnout, stress, anxiety, empathy, and depression (see Lamothe et al. 2015 for systematic review).
When considering the role of mindfulness training and activities in increasing mindfulness among genetic counselors, it is important to look at our finding that self-reported meditation, yoga, and breathing exercises were not significantly associated with mindfulness. There are several potential explanations for this. One possible explanation is methodological; in aiming to measure mindfulness-promoting activities, we may not have operationalized them effectively. Previous authors have acknowledged difficulties in measurement of such activities (Carmody and Baer 2007; Irving et al. 2009; Shapiro et al. 2006, 2008). Furthermore, we did not measure frequency, duration, or the specific nature of the activity. Thus, the lack of association between self-reported mindfulness activities and mindfulness may be a measurement issue. Alternatively, it may be attributable to heterogeneity within the reported activities and the fact that a subset lack the specificity, frequency, duration, or efficacy needed to increase mindfulness.
Increases in mindfulness appear to be sensitive to the specificity of training activities (Soler et al. 2014). Yoga and even meditation have become increasingly popular in our culture (Clarke et al. 2015), yet there is marked heterogeneity in how they are performed and they are not necessarily always done in such a way that actually develops mindfulness. In fact, the creators of MBSR have recently called for care in ensuring the fidelity of the program, given the explosion of interest in mindfulness in both clinical and popular settings (Crane et al. 2016). While we did not observe an association between mindfulness and self-reported yoga, meditation and breathing exercises, we are encouraged by the large numbers of genetic counselors who are involved in these activities (half of our sample). This involvement suggests an interest in such activities and likely an openness to mindfulness training. That, combined with the efficacy of previously studied mindfulness training, bodes well for the application of mindfulness to the genetic counseling profession.
Incorporating Mindfulness into Genetic Counselor Training
Considering the potential implications for retention, professional satisfaction and the quality of patient care, we propose that mindfulness training could be a unique and efficacious intervention for genetic counselors. Given the wealth of data supporting the efficacy of MBSR and its use in training other healthcare providers, it would be the most promising form of mindfulness training to use. Two possibilities exist for its use in the genetic counseling profession: continuing education for practicing genetic counselors, and incorporation into genetic counseling training programs.
In terms of practicing genetic counselors, it would be beneficial to implement mindfulness training into continuing education programs and/or workplace settings. As mentioned above, mindfulness training has the potential to address a significant goal of the current NSGC Strategic Plan by improving retention and clinical care in the face of increased demand for our services. Therefore, continuing education, which is endorsed by NSGC and is thought to build on a person’s expertise in a given field, seems like an ideal platform to incorporate mindfulness training. Additionally, employers may find it both advantageous and cost-effective to incorporate mindfulness training in their workplace. Research among physicians has indicated that the economic burden of one faculty departure ranges from $100,000 to $600,000 (Schloss et al. 2009). While the cost of loss of a genetic counselor has not been investigated, extrapolation of these data on physicians to genetic counselors would suggest employers stand to lose a fair amount by losing a genetic counselor. Mindfulness training may be a cost-effective method for employers to avoid the financial cost of decreased retention.
We suspect that mindfulness training could promote the Accreditation Council for Genetic Counseling (ACGC) practice-based competencies simply by raising students’ self-awareness and facilitating their ability to engage in empathic interactions. Select practice-based competencies that may be particularly impacted by mindfulness training are outlined in Table 3. A recent study found 80% of US medical schools and their affiliated universities offer mindfulness activities and that nearly one in every four medical schools in the USA has an associated mindfulness center (Barnes et al. 2016). It is possible that genetic counseling training programs, many of which are co-located with medical schools, could use these resources to promote the integration of mindfulness training into the curriculum. Essentially, the necessary institutional expertise for mindfulness training is accessible to genetic counselors at most institutions.
One argument against MBSR training is its time requirement and intensity. There have been a variety of studies examining abridged MBSR training programs (Carmody and Baer 2009). Among marriage and family therapist trainees, mental health professionals, nurses, and first-year medical students, shortened MBSR courses still demonstrate significant positive outcomes (Dobie et al. 2016; Gauthier et al. 2015; Gehart and McCollum 2008). It is possible that these abridged courses could be a feasible method for incorporating mindfulness training into genetic counselor education. However, there is also some data that suggests that the extent of improvement in outcomes depends on the length of time spent on mindfulness training (Parsons et al. 2017). Given such data and our findings, investment in the full MBSR protocol may be worthwhile.
Strengths and Limitations
Our study has several strengths: (1) a large sample size (over 400 individuals), (2) demographics representative of the overall genetic counseling profession, (3) the use of standardized measures that have proven to be valid in a variety of other studies, and (4) this is the first study to assess mindfulness among genetic counselors.
One limitation of our study is that we did not control for any potential confounding variables. While we blinded the study topic of “mindfulness” in the initial recruitment email, 50% of our study sample reported participation in mindfulness activities, which may demonstrate a positive bias toward mindfulness in our sample. We also did not determine whether participants had participated in formal mindfulness training programs. The use of a cross-sectional study design only allows identification of correlations and does not allow us to assess cause-and-effect relationships. However, our findings are situated within a large body of literature that includes many intervention studies that show improvement in both mindfulness and our key outcomes following mindfulness training. We also did not measure the ultimate outcomes that we are interested in—retention in the genetic counselor workforce, quality of patient care, and patient outcomes. Prior studies support implications for retention and quality of patient care (Bernhardt et al. 2009; Cohen-Katz et al. 2005; Coomber and Louise Barriball 2007; Duchemin et al. 2015; Grepmair et al. 2007; Haas et al. 2000; Hayes et al. 2006; Hu et al. 2012; Okie 2008; Kearney et al. 2009; Krasner et al. 2009; Shanafelt et al. 2002; Shapiro et al. 2007; Williams et al. 2010; Van Bogaert et al. 2013). As previously discussed, we may not have effectively operationalized mindfulness activities (including assessment of nature, duration, frequency). Lastly, we conducted multiple univariate tests without controlling for family wise error, which increases the likelihood of a type 1 error. However, this risk is diminished by the fact that our analysis was guided by a specific and small set of pre-defined hypotheses, and that the hypothesized and observed relationships have been reported multiple times in prior studies.
Research Recommendations
It is essential that researchers specifically inspect which mindfulness activities lead to increased mindfulness levels and the dose necessary to improve mindfulness. This will allow for more standardized and consistent measurement of such activities as well as more efficient and effective interventions aiming to increase mindfulness. Within the genetic counseling field in particular, we recommend intervention studies using MBSR training among practicing genetic counselors and students. It may also be valuable to study how the frequency and continuity of training may impact outcomes; it would be beneficial to study the impact of an intensive weekend program versus a typical eight-week MBSR program, and the need for refresher courses. Additionally, it would be helpful to assess program directors’ and students’ attitudes toward implementing MBSR training into genetic counseling curriculum to further evaluate potential benefits and barriers. Lastly, it could also be fruitful to investigate the economic burden of burnout and limited retention in genetic counseling and the cost-effectiveness of mindfulness as a preventative tool.
Conclusion
While prior research in other healthcare professions suggests that mindfulness can lead to important professional and clinically relevant benefits, this is the first study to address mindfulness among genetic counselors. We identified beneficial associations between mindfulness and key professional outcomes that have the potential to promote professional well-being, combat retention issues, and improve patient outcomes (Fig. 2). These findings are of major importance currently, as the field of genetic counseling experiences tremendous growth in demand, leading to increased professional pressures. The addition of mindfulness training to the graduate and continuing education of genetic counselors may have benefit for genetic counselors as individuals, the growth and stability of the profession as a whole, and, ultimately, the clients and families that we serve.
References
Asuero, A.M., Queralto, J. M., Pujol-Ribera, E., Berenguera, A., Rodriguez-Blanco, T., & Epstein, R. M. (2014). Effectiveness of a mindfulness educationprogram in primary health care professionals: a pragmatic controlled trial. The Journal of Continuing Education in the Health Professions, 34(1), 4–12.
Barbosa, P., Raymond, G., Zlotnick, C., Wilk, J., Toomey 3rd, R., & Mitchell 3rd, J. (2013). Mindfulness-based stress reduction training is associated with greater empathy and reduced anxiety for graduate healthcare students. Education and Health, 26(1), 9–14.
Barnes, N., Hattan, P., Black, D. S., & Schuman-Olivier, Z. (2016). An examination of mindfulness-based programs in US medical schools. Mindfulness, 8(2), 489–494.
Bazarko, D., Cate, R. A., Azocar, F., & Kreitzer, M. J. (2013). The impact of an innovative mindfulness-based stress reduction program on the health and well-being of nurses employed in a corporate setting. J Workplace Behav Health, 28(2), 107–133.
Beckman, T. J., Reed, D. A., Shanafelt, T. D., & West, C. P. (2012). Resident physician well-being and assessments of their knowledge and clinical performance. Journal of General Internal Medicine, 27(3), 325–330.
Beddoe, A. E., & Murphy, S. O. (2004). Does mindfulness decrease stress and foster empathy among nursing students? Journal of Nursing Education, 43(7), 305–312.
Benoit, L. G., Veach, P. M., & LeRoy, B. S. (2007). When you care enough to do your very best: genetic counselor experiences of compassion fatigue. Journal of Genetic Counseling, 16(3), 299–312.
Bernhardt, B. A., Rushton, C. H., Carrese, J., Pyeritz, R. E., Kolodner, K., & Geller, G. (2009). Distress and burnout among genetic service providers. Genetics in Medicine, 11(7), 527–535.
Bernhardt, B. A., Silver, R., Rushton, C. H., Micco, E., & Geller, G. (2010). What keeps you up at night? Genetics professionals’ distressing experiences in patient care. Genetics in Medicine, 12(5), 289–297.
Birnie, K., Speca, M., & Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (MBSR). Stress and Health, 26(5), 359–371.
Bishop, S. R. (2002). What do we really know about mindfulness-based stress reduction. Psychosomatic Medicine, 64, 71–84.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84, 822–848.
Caldwell, K. L. (2012). Mindfulness matters: practices for counselors and counselor education. American Counseling Association VISTAS project, 1, 1–9.
Carmody, J., & Baer, R. A. (2007). Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31(1), 23–33.
Carmody, J., & Baer, R. A. (2009). How long does a mindfulness-based stress reduction program need to be? A review of class contact hours and effect sizes for psychological distress. Journal of Clinical Psychology, 65(6), 627–638.
Clarke T.C., Black L.I., Stussman B.J., Barnes P.M., Nahin R.L. (2015). Trends in the use of complementary health approaches among adults: United States, 2002–2012. National health statistics reports; no 79. Hyattsville: National Center for Health Statistics.
Cohen-Katz, J., Wiley, S. D., Capuano, T., Baker, D. M., & Shapiro, M. A. S. (2005). The effects of mindfulness-based stress reduction on nurse stress and burnout, part II. Holistic Nursing Practice, 18(6), 26–35.
Connelly, J. (1999). Being in the present moment: developing the capacity for mindfulness in medicine. Academic Medicine, 74, 420–424.
Coomber, B., & Louise Barriball, K. (2007). Impact of job satisfaction components on intent to leave and turnover for hospital-based nurses: a review of the research literature. International Journal of Nursing Studies, 44(2), 297–314.
Costa, P., Carvalho-Filho, M. A., Schweller, M., Thiemann, P., Salgueira, A., Benson, J., et al. (2017). Measuring medical students’ empathy. Academic Medicine, 92(6), 860–867.
Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M., & Kuyken, W. (2016). What defines mindfulness-based programs? The warp and the weft. Psychological Medicine, 47(06), 990–999.
Davis, M. H. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology, 10, 85.
Davis, M. H. (1983). Measuring individual differences in empathy: evidence for a multidimensional approach. Journal of Personality and Social Psychology, 44, 113–126.
Davis, C. M. (1990). What is empathy, and can empathy be taught? Physical Therapy, 70(11), 707–711.
Dobie, S. (2007). Viewpoint: reflections on a well-traveled path: self-awareness, mindful practice, and relationship-centered care as foundations for medical education. Academic Medicine, 82(4), 422–427.
Dobie, A., Tucker, A., Ferrari, M., & Rogers, J. M. (2016). Preliminary evaluation of a brief mindfulness-based stress reduction intervention for mental health professionals. Australasian Psychiatry, 24(1), 42–45.
Duchemin, A., Steinberg, B. A., Marks, D. R., Vanover, K., & Klatt, M. (2015). A Small Randomized Pilot Study of a Workplace Mindfulness-Based Intervention for Surgical Intensive Care Unit Personnel. Journal of Occupational and Environmental Medicine, 57(4), 393–399.
Epstein, R. M. (1999). Mindful practice. JAMA, 282(9), 833–839.
Gauthier, T., Meyer, R. M. L., Grefe, D., & Gold, J. I. (2015). An on-the-job mindfulness-based intervention for pediatric ICU nurses: a pilot. Journal of Pediatric Nursing, 30(2), 402–409.
Gehart, D. R., & McCollum, E. E. (2008). Teaching therapeutic presence: a mindfulness-based approach. In S. Hick & T. Bien (Eds.), Mindfulness and the therapeutic relationship (pp. 176–194). New York: Guilford.
Geller, G., Rushton, C. H., Francomano, C., Kolodner, K., & Bernhardt, B. A. (2010). Genetics professionals’ experiences with grief and loss: implications for support and training. Clinical Genetics, 77(5), 421–429.
Goodman, M. J., & Schorling, J. B. (2012). A mindfulness course decreases burnout and improves well-being among healthcare providers. International Journal of Psychiatry in Medicine, 43(2), 119–128.
Gotink, R. A., Chu, P., Busschbach, J. J., Benson, H., Fricchione, G. L., & Hunink, M. G. (2015). Standardised Mindfulness-Based Interventions in Healthcare: An Overview of Systematic Reviews and Meta-Analyses of RCTs. Plos One, 10(4). https://doi.org/10.1371/journal.pone.0124344.
Grepmair, L., Mitterlehner, F., Loew, T., Bachler, E., Rother, W., & Nickel, M. (2007). Promoting mindfulness in psychotherapists in training influences the treatment results of their patients: a randomized, double-blind, controlled study. Psychotherapy and Psychosomatics, 76(6), 332–338.
Haas, J. S., Cook, E. F., Puopolo, A. L., Burstin, H. R., Cleary, P. D., & Brennan, T. A. (2000). Is the professional satisfaction of general internists associated with patient satisfaction? Journal of General Internal Medicine, 15(2), 122–128.
Halpern, J., (2003). What is clinical empathy?. Journal of General Internal Medicine, 18(8), 670–674
Hayes, L. J., O’Brien-Pallas, L., Duffield, C., Shamian, J., Buchan, J., Hughes, F., Spence Laschinger, H. K., North, N., & Stone, P. W. (2006). Nurse turnover: a literature review. International Journal of Nursing Studies, 43(2), 237–263.
Hu, Y., Fix, M. L., Hevelone, N. D., Lipsitz, S. R., Greenberg, C. C., Weissman, J. S., & Shapiro, J. (2012). Physicians needs in coping with emotional stressors. Archives of Surgery, 147(3), 212–217.
Injeyan, M. C., Shuman, C., Shugar, A., Chitayat, D., Atenafu, E. G., & Kaiser, A. (2011). Personality traits associated with genetic counselor compassion fatigue: the roles of dispositional optimism and locus of control. Journal of Genetic Counseling, 20, 526–540.
Irving, J. A., Dobkin, P. L., & Park, J. (2009). Cultivating mindfulness in health care professionals: a review of empirical studies of mindfulness-based stress reduction (MBSR). Complementary Therapies in Clinical Practice, 15, 61–66.
Kabat-Zinn, J. (1994). Wherever you go there you are: mindfulness meditation in everyday life. New York: Hyperion.
Kearney, M. K., Weininger, R. B., Vachon, M. L. S., Harrison, R. L., & Mount, B. M. (2009). Self-care of physicians caring for patients at the end of life: “Being connected...a key to my survival.”. JAMA, 301(11), 1155–1164.
Kesbakhi, M. S., Rohani, C., Mohtashami, J., & Nasiri, M. (2017). Empathy from the perspective of oncology nurses. Journal of Compassionate Health Care., 4(7), 1–10.
Kiosses, V. N., Karathanos, V. T., & Tatsioni, A. (2016). Empathy promoting interventions for health professionals: a systematic review of RCTs. Journal of Compassionate Health Care, 3(1).
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302(12), 1284–1293.
Kunie, K., Kawakami, N., Shimazu, A., Yonekura, Y., & Miyamoto, Y. (2017). The relationship between work engagement and psychological distress of hospital nurses and the perceived communication behaviors of their nurse managers: a cross-sectional survey. International Journal of Nursing Studies, 71, 115–124.
Lamothe, M., Rondeau, É., Malboeuf-Hurtubise, C., Duval, M., & Sultan, S. (2015). Outcomes of MBSR or MBSR-based interventions in health care providers: a systematic review with a focus on empathy and emotional competencies. Complementary Therapies in Medicine, 24, 19–28.
Lamothe, M., Mcduff, P., Pastore, Y. D., Duval, M., & Sultan, S. (2018). Developing professional caregivers’ empathy and emotional competencies through mindfulness-based stress reduction (MBSR): results of two proof-of-concept studies. BMJ Open, 8(1). https://doi.org/10.1136/bmjopen-2017-018421.
Lee, W., Veach, P. M., Macfarlane, I. M., & Leroy, B. S. (2015). Who is at risk for compassion fatigue? An investigation of genetic counselor demographics, anxiety, compassion satisfaction, and burnout. Journal of Genetic Counseling, 24, 358–370.
Loerbroks, A., Glaser, J., Vu-Eickmann, P., & Angerer, P. (2017). Physician burnout, work engagement and the quality of patient care. Occupational Medicine, 67(5), 356–362.
Meiser, B., Irle, J., Lobb, E., & Barlow-Stewart, K. (2008). Assessment of the content and process of genetic counseling: a critical review of empirical studies. Journal of Genetic Counseling, 17(5), 434–451.
National Society of Genetic Counselors (NSGC). (2016). Professional Status Survey. Retrieved May 13, 2016, from https://www.nsgc.org/p/cm/ld/fid=68.
Okie, S. (2008). Innovation in primary care—staying one step ahead of burnout. The New England Journal of Medicine, 359(22), 2305–2309.
Pan, V., Yashar, B. M., Pothast, R., & Wicklund, C. (2016). Expanding the genetic counseling workforce: program directors’ views on increasing the size of genetic counseling graduate programs. Genetics in Medicine, 18(8), 842–849.
Parsons, C. E., Crane, C., Parsons, L. J., Fjorback, L. O., & Kuyken, W. (2017). Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants mindfulness practice and its association with outcomes. Behaviour Research and Therapy, 95, 29–41.
Ruff, K. M., & Mackenzie, E. R. (2009). The role of mindfulness in healthcare reform: a policy paper. EXPLORE: The Journal of Science and Healing, 5(6), 313–323.
Santorelli S.F., Kabat-Zinn J., Blacker M., Meleo-Meyer F., & Koerbel L. (eds) (2017) Mindfulness-Based Stress Reduction (MBSR) Authorized Curriculum Guide (http://www.umassmed.edu/cfm/training/mbsr-curriculum).
Schaufeli, W. B., & Bakker, A. B. (2003). UWES Utrecht work engagement scale preliminary manual. Journal of Occupational Health Psychology, 58.
Schaufeli, W. B., Bakker, A. B., & Salanova, M. (2006). The measurement of short questionnaire: a cross-national study. Educational and Psychological Measurement, 66(4), 701–716.
Schloss, E. P., Flanagan, D. M., Culler, C. L., & Wright, A. L. (2009). Some hidden costs of faculty turnover in clinical departments in one academic medical center. Academic Medicine, 84(1), 32–36.
Shanafelt, T. D. (2009). Enhancing meaning in work: a prescription for preventing physician burnout and promoting patient-centered care. JAMA, 302(12), 1338–1340.
Shanafelt, T. D., Bradley, K. A., Wipf, J. E., & Back, A. L. (2002). Burnout and self-reported patient care in an internal medicine residency program. Annals of Internal Medicine, 136(5), 358–367.
Shapiro, S. L., Brown, K. W., & Biegel, G. M. (2007). Teaching self-care to caregivers: effects of mindfulness-based stress reduction on the mental health of therapists in training. Training and Education in Professional Psychology, 1(2), 105–115.
Shapiro, S. L., Carlson, L. E., Astin, J. A., & Freedman, B. (2006). Mechanisms of mindfulness. Journal of Clinical Psychology, 26(3), 373–386.
Shapiro, S. L., Oman, D., Thoresen, C. E., Plante, T. G., & Flinders, T. (2008). Cultivating mindfulness: effects on well-being. Journal of Clinical Psychology, 64(7), 840–862.
Shapiro, S. L., Schwartz, G. E., & Bonner, G. (1998). Effects of mindfulness-based stress reduction on medical and premedical students. Journal of Behavioral Medicine, 21(6), 581–600.
Soler, J., Cebolla, A., Feliu-Soler, A., Demarzo, M. M. P., Pascual, J. C., & Bañía-Campayo, J. (2014). Relationship between meditative practice and self-reported mindfulness: the MINDSENS composite index. PLoS One, 9(1), e86622.
Stahl, B., & Goldstein, E. (2010). A mindfulness-based stress reduction workbook. Oakland: New Harbinger.
Stamm, B. (2010). The Concise ProQOL Manual. Pocatello, ID: ProQOL. Org, 78. Retrieved from http://proqol.org/uploads/ProQOL_Concise_2ndEd_12-2010.pdf
Udipi, S., Veach, P. M., Kao, J., & Leroy, B. S. (2008). The psychic costs of empathic engagement: personal and demographic predictors of genetic counselor compassion fatigue. Journal of Genetic Counseling, 17, 459–471.
Van Bogaert, P., Wouters, K., Willems, R., Mondelaers, M., & Clarke, S. (2013). Work engagement supports nurse workforce stability and quality of care: nursing team-level analysis in psychiatric hospitals. Journal of Psychiatric and Mental Health Nursing, 20(8), 679–686.
Van Mol, M. M., Nijkamp, M. D., Bakker, J., Schaufeli, W. B., & Kompanje, E. J. (2017). Counterbalancing work-related stress? Work engagement among intensive care professionals. Australian Critical Care. https://doi.org/10.1016/j.aucc.2017.05.001.
Veach, P. M., Bartels, D. M., & LeRoy, B. S. (2007). Coming full circle: a reciprocal-engagement model of genetic counseling practice. Journal of Genetic Counseling, 16(6), 713–728.
Veach, P. M., LeRoy, B. S., & Bartels, D. M. (2003). Listening to clients: primary empathy skills. In Facilitating the genetic counseling process: a practice manual (pp. 51–53). New York: Springer-Verlag.
Weil, J. (2000). Techniques of psychosocial genetic counseling. In Psychosocial genetic counseling (pp. 53–55). New York: Oxford University Press.
Williams, E. S., Konrad, T. R., Scheckler, W. E., Pathman, D. E., Linzer, M., McMurray, J. E., Gerrity, M., & Schwartz, M. (2010). Understanding physicians’ intentions to withdraw from practice. Health Care Management Review, 35(2), 105–115.
Wiseman, T. (1996). A concept analysis of empathy. Journal of Advanced Nursing, 23, 1162–1167.
Zwack, J., & Schweitzer, J. (2013). If every fifth physician is affected by burnout, what about the other four? Resilience strategies of experienced physicians. Academic Medicine, 88(3), 382–389 Retrieved September 28, 2017.
Acknowledgments
This study was completed in partial fulfillment of the requirements for the first author’s Master of Science degree from the Stanford University. We are grateful to the genetic counselors who participated in this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Julia Silver, Colleen Caleshu, Kelly Ormond and Sylvie Casson-Parkin declare that they have no conflict of interest.
Human Studies and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients for being included in the study.
Animal Studies
No animal or human studies were carried out by the authors for this article.
Electronic supplementary material
ESM 1
(PDF 91.0 kb)
Rights and permissions
About this article

Cite this article
Silver, J., Caleshu, C., Casson-Parkin, S. et al. Mindfulness Among Genetic Counselors Is Associated with Increased Empathy and Work Engagement and Decreased Burnout and Compassion Fatigue. J Genet Counsel 27, 1175–1186 (2018). https://doi.org/10.1007/s10897-018-0236-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-018-0236-6