
Abstract
Self-help may help fill the large treatment gap in individuals with body-focused repetitive behaviors (BFRBs). We examined the efficacy of three self-help techniques for BFRBs: habit reversal training (HRT), decoupling (DC), and decoupling in sensu (DC-is) and also tested whether a video demonstration is more efficacious to written instructions. A total of 224 participants with at least one BFRB were randomly assigned to two intervention groups (video, manual) receiving access to all techniques or a wait-list control group (1:1:1). A 6-week follow-up assessment was conducted. The Generic Body-Focused Repetitive Behavior Scale (GBS-9) served as primary outcome. The intention-to-treat analysis showed significant improvements for the manual group compared to the wait-list control group on GBS total score and severity and impairment scores. For the per-protocol analyses (i.e., participants had at least read/watched the manual/video), 26.9% of completers in the manual group improved at least 35% in GBS compared to 23.3% (video group) and 15.9% (control). A dose–response relationship emerged for the video group. Subjective ratings by the video and manual groups did not differ; treatment satisfaction was greater for HRT and DC than for DC-is. Results suggest that the manual group showed somewhat stronger effects than the video group when usage frequency was low. With more frequent usage, improvements in the video condition increased. Future studies should investigate potential order effects of the techniques as well as add-on effects when techniques are used along with other treatment approaches.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Body-focused repetitive behaviors (BFRBs) such as trichotillomania, nail biting, skin picking, and lip/cheek biting are characterized by the inability to reduce or stop behaviors that target one’s own body, usually manifesting in the (forceful) removal of body parts such as fingernails, hair, or skin (APA, 2013; Teng et al., 2002).
BFRBs are common but remain largely under-researched and under-treated. In a study of 4335 students, approximately 59% reported the presence of BFRBs and 12% met diagnostic criteria (Houghton et al., 2018). Comorbidity of two or more BFRB conditions is high (Frydman et al., 2017; Houghton et al., 2018; Solley & Turner, 2018).
Psychological treatments such as habit reversal training (HRT) show some efficacy (Flessner et al., 2008; Keuthen et al., 2012; McGuire et al., 2014; Woods et al., 2006). Promising results have also been reported for dialectical behavior therapy (DBT)-enhanced HRT (Keuthen et al., 2012), comprehensive behavioral treatment (COMB; Carlson et al., 2021) and acceptance and commitment therapy (Lee et al., 2020). While psychopharmacological treatments also show merit in some individuals, no medication has yet been approved by the Food and Drug Administration (Falkenstein, 2016; Grant, 2016).
Yet, effective treatments are rarely adopted as many with a BFRB do not seek or receive treatment (Gallinat et al., 2019; Siddiqui et al., 2017; Tucker et al., 2011; Weingarden & Renshaw, 2015). In addition, relapse rates are quite high (Falkenstein, 2016; Falkenstein et al., 2014; Skurya et al., 2020).
Recently, our research group created three self-help versions for three techniques that showed some efficacy in subsequent research: self-help HRT (Moritz et al., 2012), decoupling (DC; Moritz & Rufer, 2011; Moritz et al., 2011, 2020a, 2020b), and decoupling in sensu (DC-is; Moritz et al., 2020a, 2020b, 2021). The first technique was initially created by Azrin and Narens (1973) as a therapist-guided intervention, and the latter two were developed by the authors. Only two head-to-head comparisons have been conducted. In the first study (Moritz et al., 2012), the efficacy of self-help HRT was compared against decoupling in individuals suffering from skin picking. Although symptom reduction was found in both interventions, decoupling was less effective (Moritz et al., 2012). A recent study (Moritz et al., 2021) compared the three self-help techniques against each other in a sample of 113 participants in the framework of a randomized controlled trial (RCT). In terms of recovery rate, subjective appraisals, and objective symptom improvement, decoupling in sensu showed the best results. HRT yielded good subjective but less objective improvement.
Emotional and motivational processes play a key role in learning new alternative behaviors and likely impact the effectiveness of treatments. The medium used to present the content has a significant impact on a person’s motivation or emotions. When watching a video, for example, the level of involvement or immersion as well as the level of commitment seems to be higher than when the content is conveyed via text (Syring et al., 2015). Additionally, individuals who have watched a video enjoy learning what is presented more than individuals reading the same content (Koehler et al., 2005; Syring et al., 2015). Learning performance and satisfaction also improve with video usage (Berney & Bétrancourt, 2016; Noetel et al., 2021; Stockwell et al., 2015). In particular, animated visualizations seem to be more effective than pictures for the acquisition of procedural motor skills (Höffler & Leutner, 2007), and the use of videos seems to facilitate content comprehension (Council for Cultural Education, 2019). In the clinical/psychotherapeutic context, there is preliminary evidence for the effectiveness of video interventions for some disorders (Mason et al., 2012; see also Ozcan & Merdan, 2020).
The present study was designed to compare the effectiveness of the three self-help techniques for different BFRBs against a control group. The techniques were conveyed via either a video or a manual in order to examine differences in treatment outcomes. In contrast to the pilot study by Moritz et al. (2021), we also implemented a wait-list control group. Considering the previously described research findings, we hypothesized that both the manual and the video group would show greater improvement than the wait-list control group and that the video would be more effective than the manual.
Methods
Sample
Individuals from German-speaking countries aged between 18 and 75 years and reporting one or more BFRBs (e.g., trichotillomania) were eligible to participate in the study. Further criteria for participation were the ability to provide informed consent and the availability of internet access. Participants were also required to participate in two anonymous online surveys, each lasting approximately 25 to 30 min. Participants were recruited through advertisements and posts in online self-help forums (e.g., Facebook groups) as well as through the German Society for Obsessive–Compulsive Disorders (DGZ).
At the beginning of the sample acquisition, the optimal sample size was determined using G*Power. Given the error level for the type I error (α = 0.05; power = 0.8), and a medium to strong effect size (v/f = 0.5), the program indicated an optimal sample size of 64 participants per group. To ensure a sufficiently large sample, taking into account potential dropout, a sample size of 70 participants in each of the three conditions was targeted (N = 210).
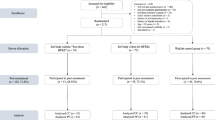
Exclusions included individuals who did not meet the previously defined age criterion (< 18 and > 75 years; n = 5). Subjects with acute suicidal intentions (n = 3) and/or schizophrenia (n = 3) were also excluded from participation in the study. The final sample consisted of 224 participants (video group: n = 69; manual group: n = 73; wait-list control group: n = 82; the flow chart is available by email upon request).
Study Design
A randomized controlled trial (RCT) was conducted in which the self-help techniques habit reversal training (HRT), decoupling (DC), and decoupling in sensu (DC-is) were compiled into one document so that participants received all three techniques. The techniques were conveyed via either text or video; both forms of the intervention provided the same content.
At the end of the baseline survey, participants were asked to provide an anonymous email address so that no personal identification was possible (the email address entered at baseline was requested again in the follow-up survey to match participants). After the baseline survey, participants were automatically randomized to one of three conditions (1:1:1). These were the two intervention groups (manual, video) and a wait-list control group. Participants in the intervention groups received immediate access to the video or manual via email.
During the 6-week intervention period, participants in the intervention groups had to practice the self-help techniques on their own. Participants in the control group received no treatment but were allowed to continue their previously scheduled therapy. After the intervention period, all participants were automatically invited by email to participate in the follow-up survey (up to three reminders were sent). As incentive for participation in the final survey, participants were offered two additional self-help tools (the COGITO app, a mobile-based intervention to reduce emotional problems and a manual on progressive muscle relaxation), and all received access to both the self-help video and the self-help manual after post-assessment.
Intervention
The manual totaled 12 pages (the most recent version can be retrieved at no cost from www.free-from-bfrb.org). The video had a total length of about 17 min. The video group had access to the full-length video but could also watch the individual techniques in separate videos. Both the self-help manual and the video were divided into a psychoeducational section and a section explaining the three techniques in more detail. The initial psychoeducation section conveyed evidence-based knowledge regarding different BFRBs and frequent adverse consequences. Then, the section ‘Observing/keeping a log of your unwanted behavior’ encouraged awareness. In the next sections, the individual techniques were explained. HRT was described first, followed by DC and then DC-is. The explanation of each technique was followed by instructions for practice with examples. It was emphasized that the individual techniques should be performed one after the other and not in parallel.
Habit reversal training (HRT) includes several components; the core elements are awareness training and competing response training (CRT) (Azrin & Nunn, 1973). In CRT, the individual performs a behavior that is incompatible with the problem behavior, thereby preventing it from occurring. Typically, a ‘rigid/frozen’ behavior (e.g., clenching a fist) is carried out with a certain amount of tension. This alternative behavior is to be used whenever the problem behavior itself occurs or when its precursors are apparent.
The technique of decoupling (DC) represents a variant of HRT (Moritz & Rufer, 2011). In this process, the habitual behavior pattern is first imitated. Just before performing the original dysfunctional behavior, the behavioral target is shifted and the movement is transformed into an innocuous behavior (i.e., targeting another body part or a specific point in space). The final movement is executed with some acceleration and tension.
Decoupling in sensu (DC-is) is a variant of DC (Moritz et al., 2021). In contrast to DC, the imitation of the original misbehavior takes place only in the imagination. Shortly before the undesired behavior occurs in the imagination, the imagined movement is interrupted by a real movement (e.g., the imagined hand moving toward the mouth is interrupted by an actual movement of the hand toward the ear shortly before the imagined hand reaches the mouth). DC-is is thought to produce greater generalization than conventional decoupling because the individual only imagines the problematic behavior and thus no specific motor pattern is reinforced (Moritz et al., 2020a, 2020b). The accelerated movement of the alternative behavior is also thought to help disrupt and overwrite the old movement pattern (Moritz et al., 2021).
We asked participants to choose among the techniques they liked best or the rationale they found the most persuasive. This is not uncommon in self-help books, where a number of different techniques are often conveyed without a clear explanation given for the order in which to apply them.
Habit reversal training is based on the assumption that resisting an urge may not just postpone the urge but may even cause it to eventually subside. The technique necessitates awareness of one’s triggers because without this awareness, the individual cannot change their behavior. The rationale for DC and DC-is is different; the urge to perform a harmful behavior is redirected to a benign behavior so that triggers such as stress do not result in the execution of the dysfunctional behavior.
Acquisition
The study was approved by the Ethics Committee of the University Medical Center Hamburg-Eppendorf (Germany; LPEK-0254), and it was pre-registered with the German Register of Clinical Trials (DRKS; DRKS00024478).
First, sociodemographic data (gender, age), lifetime prevalence of BFRBs, prevalence of BFRBs in the previous 2 weeks, and treatment experiences including current medication were asked for in the baseline survey. We then presented the questionnaires described below. In the follow-up survey, participants were also asked about the extent to which they had used the manual/video on a 7-point scale from ‘not read/watched’ (1) to ‘used several times a day’ (7).
Primary Outcome
The primary outcome was the Generic Body-Focused Repetitive Behavior Scale (GBS-9). Our scale was derived from the eight items of the Skin Picking Scale-Revised (SPS-R; Snorrason et al., 2012). This scale is slightly reformulated to capture different forms of BFRBs (Moritz et al., 2021). The observation period was restricted to the previous 2 weeks (baseline) or the previous week (post-assessment; Moritz et al., 2021).
The items of the GBS-9 are rated on a 5-point Likert scale from 0 to 4 (e.g., item ‘ability to control the urge’: ‘no urge/could always control the urge’ (0) to ‘urge hardly/not at all controllable’ (4); Moritz et al., 2021). Two subscales (symptom severity and impairment) and a total score can be calculated. The symptom severity subscale is composed of the sum of items 1, 2, and 4 (frequency urge, intensity urge, frequency) and the mean of items 3 and 5 (ability control, control). The impairment subscale is formed by the sum of items 6 through 9 (suffering, impairment, avoidance, actual consequences; Moritz et al., 2021). According to Moritz et al. (2021), the GBS-9 has satisfactory test–retest reliability for the total score (r = 0.760, p < 0.001).
Secondary Outcomes
World Health Organization Quality of Life – BREF (WHOQOL-BREF)
The global item of the World Health Organization Quality of Life – BREF (WHOQOL-BREF; The WHOQOL Group, 1998) was used to estimate quality of life. The global item captures general perceptions of quality of life with a 5-point Likert scale.
Patient Health Questionnaire-9 (PHQ-9)
The self-assessment questionnaire PHQ-9 was used to measure depressive symptoms in the previous week (Kroenke et al., 2001). The PHQ-9 has good psychometric properties (Kroenke et al., 2001).
Other Measurements
Participants who at least read/watched the manual/video were asked to answer the Client Satisfaction Questionnaire (CSQ-8; Schmidt et al., 1989). The CSQ-8 assessed subjective appraisal of the video as well as of the manual (e.g., quality, satisfaction, subjective efficacy, intention to use in the future). The efficacy of each technique was measured in the follow-up survey using another self-report questionnaire that addresses the usefulness, comprehensibility, and application of the techniques described in the video or manual.
Statistical Analysis
For the analysis of the primary and secondary outcomes, a mixed ANOVA was carried out, with group (control, video, and manual) as between-subjects factor and time (baseline and follow-up assessments) as within-subjects factor. Significant interaction effects were tested by post-hoc tests (least significant difference).
An intention-to-treat (ITT) analysis was performed in which missing values were estimated using the expectation–maximization (EM) method. Complete case (CC) and per-protocol (PP) analyses were also performed. The CC analysis included all participants with available baseline data and post-data, but the PP analyses included only those who had at least read/watched the manual/video and completed the follow-up survey. For the secondary exploratory analyses, we conducted additional analyses of variance, t-tests, chi-square tests, and correlation analyses.
Results
Sample Characteristics
The groups did not differ significantly in any sociodemographic or psychopathological variables at baseline (see Table 1). The mean age of the study participants was early 30s; approximately 80% of the participants in each group were female. About half of the participants had no other psychiatric diagnoses (based on self-report). Depression was reported in one third of the cases (33%), obsessive–compulsive disorder in less than one eighth (12.1%). At the time of the baseline survey, skin picking was most frequent in the sample, followed by nail biting, trichotillomania, and lip/cheek biting (cavitadaxia). Participants had a mean total of 1.58 BFRBs at the time of study implementation (SD = 0.75; one BFRB = 54%, two BFRBs = 32.1%, three BFRBs = 12.1%, four BFRBs = 0.9%).
Test–Retest Reliability and Internal Consistency
For the control group, test–retest reliabilities of GBS total score (r = 0.69; severity: r = 0.60; impairment: r = 0.73) and PHQ-9 depressive symptoms (r = 0.60) were acceptable to satisfactory (all p < 0.001). Reliability was low for WHOQOL-BREF quality of life (r = 0.40).
Acceptable to satisfactory internal consistency was demonstrated for all GBS (sub-)scales: severity (Cronbach’s α = 0.799), total score (Cronbach’s α = 0.821), and impairment (Cronbach’s α = 0.792).
Adherence (Participation in Pre- and Post-Assessments) and Efficacy
The completion rate was 72.5% in the video group, 75.3% in the manual group, and 76.8% in the control group (total group: 168/224, 75%; χ2(2) = 0.39, p = 0.824).
Most participants reported having at least read/watched the manual/video, with lower frequencies in the video condition (manual: 94.5%, video: 86%; χ2(1) = 2.22, p = 0.136). A total of 70.9% of the manual group performed the exercises at least once, compared to 74% in the video group (χ2(1) = 0.12, p = 0.723). A total of 47.3% of the manual and 44% of the video group performed the exercises at least once per week (χ2(1) = 0.11, p = 0.737).
A total of 67.6% performed HRT. DC was practiced by 53.3%, and DC-is was used the least, with 47.6% (no differences between manual vs. video, all ps > 0.1). Regarding the combination of techniques, 25% (manual: 15.4%, video: 35.1%) of participants in the per-protocol sample performed one technique, 17.1% (manual: 15.4%, video: 18.9%) performed two techniques, and 57.9% (manual: 69.2%, video: 45.9%) performed three techniques, with a trend for more combined usage in the manual condition (χ2(2) = 4.88, p = 0.087).
Table 2 shows the change in the severity of symptoms measured with the GBS-9 as well as quality of life and depression over time using ITT and CC analyses. ITT analysis showed that participants improved across all domains regardless of group assignment. There were statistically significant interactions between time and group for GBS total score and the severity and impairment scores at a small to medium effect size, while no significant interactions were observed for quality of life and depressive symptoms. LSD post-hoc tests revealed significant improvements in the manual group compared to the control group for GBS total score and severity and impairment scores, with small to moderate effect sizes. The video group showed no significant improvements in GBS total score or severity and impairment scores compared to the control group.
A total of three PP analyses were conducted for participants who (1) read/watched the manual/video at least once, (2) performed the technique(s) at least once, or (3) performed the technique(s) once a week. Using these analyses (available from the first author on request), the manual group showed significant improvement at low usage frequency (GBS total score in PP (1): p = 0.002, d = 0.57; GBS total score in PP (2): p = 0.010, d = 0.51; severity in PP (1): p = 0.005, d = 0.54; severity in PP (2): p = 0.013, d = 0.50) relative to the video group. However, when the techniques were performed more frequently, significant improvements were also seen in the video group relative to the control group (GBS total score in PP (3): p = 0.002, d = 0.81; severity in PP (3): p = 0.001, d = 0.93). For individuals in the video group who performed the exercises weekly, a greater improvement in symptom severity was found compared to the manual group (results available upon email request).
Subjective Appraisal of Efficacy and Feasibility
The assessments of the manual and video groups showed no significant differences. More than 80% of the participants confirmed the following statements: good or excellent quality of the manual/video, receiving the treatment originally hoped for (video only), recommending the manual/video to a friend, satisfaction with the amount of help received (video only), overall satisfaction with the manual/video (manual only), willingness to use the manual/video again.
Acceptability and subjective efficacy of the three self-help techniques were good across all conditions, with DC-is predominantly receiving the lowest ratings and HRT and DC receiving the highest ratings. There were no significant differences in ratings between the manual and video groups (data available upon email request).
Dose–Response Relationship
Correlation analyses further showed that frequency of use and total GBS score were significantly and moderately correlated in the video group (r = 0.359, p = 0.011). In the manual group, this correlation was not significant (r = 0.103, p = 0.456).
Discussion
The present study was designed to examine the efficacy of three self-help techniques (HRT, DC, DC-is) in individuals with BFRBs. We also investigated the comparative efficacy of the techniques using two different modes of presentation (a video vs. a written manual).
The results suggest that self-help techniques are a promising treatment option for a subgroup of individuals with BFRBs: Compared with 15.9% in the control group, 26.9% of participants in the manual group and 23.3% of participants in the video group who had at least read or watched the manual or video showed a minimum improvement of 35% on the Generic Body-Focused Repetitive Behavior Scale (GBS-9). There was a significant improvement in the GBS total score as well as the subscales across all conditions, which was however stronger in the experimental groups. For quality of life, however, a significant improvement was observed only in the manual group. Completion rate was satisfactory and nonsignificant across groups.
Compared to controls, only participants in the manual group showed significant improvements in the GBS total score and the severity score in the CC analysis. The video group showed only a trend toward a differentially stronger improvement compared to the control group. ITT analysis largely confirmed these results. Supplementary PP analyses showed that stronger effects occurred in the manual group than in the video group, especially at a low usage frequency of the technique(s). With increasing usage frequency, the efficacy of the video condition increased. The video condition proved to be more effective for participants who performed the technique(s) at least once a week; in this case, large effect sizes were observed.
The effect of combining techniques with treatment approaches that focus on other aspects of BFRBs should also be investigated in future studies. For example, because individuals with BFRBs often exhibit deficits in emotion regulation and the majority of these behaviors are triggered by anxiety, tension, or boredom (Roberts et al., 2016), a combination of the self-help techniques and emotion regulation strategies should be tested. Combining self-help techniques with therapist-guided treatment approaches that have already been shown to be effective when combined with HRT (acceptance-commitment therapy [ACT]: Flessner et al., 2008; Woods et al., 2006; dialectical behavior therapy [DBT]: Keuthen et al., 2012) should also be considered.
The subjective appraisal of the participants regarding the video and the manual was good in both conditions with no significant differences. More than 80% of the participants in the video condition were satisfied with the amount of help they received. In contrast to the study results of Stockwell et al. (2015) on using video elements in learning contexts, the present study showed no increased satisfaction when using a video compared to text-based content. DC and HRT achieved significantly higher overall subjective ratings than DC-is. The results are partially consistent with previous study findings. Other studies have also confirmed the efficacy of HRT for various BFRBs (Bate et al., 2011; Lee et al., 2019; Moritz et al., 2012) as well as the efficacy of the decoupling technique for trichotillomania (Moritz & Rufer, 2011) and nail biting (Moritz et al., 2011). In the present work, correlation analyses even showed that symptom reduction increased due to DC, especially for individuals with trichotillomania. For individuals with skin picking, however, previous studies have shown a lack of effectiveness of DC (Moritz et al., 2012, 2021), which contradicts the present findings: the majority of participants were affected by skin picking (66–70%) and still benefited from DC. Also, the lack of subjective efficacy of DC-is does not align with previous research findings that the technique is effective for various BFRBs, including skin picking (Moritz et al., 2020a, 2020b, 2021).
Because this was the first time all three techniques were provided to participants, the differences in subjective ratings of the techniques may reflect a primacy effect (Anderson & Barrios, 1961). In line with this, HRT—the technique described first—was performed most frequently, at approximately 67.6%. In contrast, DC-is, which was presented last, was performed by only 53.3%. It is therefore reasonable to assume that the presentation order influenced not only frequency of use but also technique ratings. Thus, when reading a manual or watching a video, a positive impression of the technique described first (HRT), which also has the greatest evidence to date, may have influenced the impression of the subsequent techniques. In addition, the successes achieved with the method performed first might have been perceived more strongly compared to those performed later. A recent study tentatively shows that effects of the techniques might be strongest when participants start using decoupling (Moritz et al, 2023).
Limitations
Some limitations need to be acknowledged. First, the majority were female (approximately 83%) and were affected by skin picking (approximately 66–70%) limiting generalizability. Second, the study results do not address the long-term efficacy of the self-help techniques as no long-term follow-up was conducted. However, this is important, especially given the high relapse rates among people suffering from BFRBs (Falkenstein, 2016; Skurya et al., 2020). Therefore, the study was unable to determine whether the improvements were long-lasting or whether some participants might show delayed changes in behavior (so-called sleeper effects; see Hannah & Sternthal, 1984). As further limitations, the diagnoses have not been validated, which is the case in many other studies; in fact, there are still no firm diagnostic criteria for BFRBs except for trichotillomania and skin picking. Another limitation to consider is the collection of information based on self-report. By informing study participants of the study’s anonymity and also asking them to create an anonymous email address, we aimed to counteract these effects. In addition, a small number of the participants performed the exercises regularly; less than 50% of the individuals from the manual group and the video group performed the exercises at least weekly.
Conclusion
In summary, the self-help techniques HRT, DC, and DC-is are promising options for bridging treatment to conventional psychotherapeutic approaches for people with BFRBs. In particular, they offer an alternative to those who are not yet seeking professional treatment due to shame or other reasons.
Although there were no differences in participant satisfaction between the video group and the manual group, stronger effects were found in the manual group than in the video group when the utilization frequency of the technique(s) was low. With more frequent practice, the efficacy of the video condition increased.
Future studies should investigate whether the order the techniques were presented in the video and the manual impacts their efficacy and whether additive effects can be observed when the techniques are used in combination with treatment approaches targeting other aspects of BFRBs. Furthermore, the use of a mobile app that regularly reminds participants to perform the exercises could also enhance their efficacy.
References
Anderson, N. H., & Barrios, A. A. (1961). Primacy effects in personality impression formation. The Journal of Abnormal and Social Psychology, 63(2), 346–350. https://doi.org/10.1037/h0046719
APA. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
Azrin, N. H., & Nunn, R. G. (1973). Habit-reversal: A method of eliminating nervous habits and tics. Behaviour Research and Therapy, 11(4), 619–628. https://doi.org/10.1016/0005-7967(73)90119-8
Bate, K. S., Malouff, J. M., Thorsteinsson, E. T., & Bhullar, N. (2011). The efficacy of habit reversal therapy for tics, habit disorders, and stuttering: A meta-analytic review. Clinical Psychology Review, 31(5), 865–871. https://doi.org/10.1016/j.cpr.2011.03.013
Berney, S., & Bétrancourt, M. (2016). Does animation enhance learning? A meta-analysis. Computers & Education, 101, 150–167. https://doi.org/10.1016/j.compedu.2016.06.005
Carlson, E. J., Malloy, E. J., Brauer, L., Golomb, R. G., Grant, J. E., Mansueto, C. S., & Haaga, D. A. F. (2021). Comprehensive behavioral (ComB) treatment of trichotillomania: A randomized clinical trial. Behavior Therapy, 52(6), 1543–1557. https://doi.org/10.1016/j.beth.2021.05.007
Council for Cultural Education. (2019). Youth/Youtube/Cultural Education—Horizon 2019 study: A representative survey of 12- to 19-year-olds on the use of cultural education offerings at digital cultural sites. Retrieved from https://www.rat-kulturelle-bildung.de/fileadmin/user_upload/pdf/Studie_YouTube_Webversion_final.pdf
Falkenstein, M. J. (2016). Clinical aspects of hair pulling, skin picking, and nail biting. Current Treatment Options in Psychiatry, 3(4), 375–384. https://doi.org/10.1007/s40501-016-0096-3
Falkenstein, M. J., Rogers, K., Malloy, E. J., & Haaga, D. A. F. (2014). Predictors of relapse following treatment of trichotillomania. Journal of Obsessive-Compulsive and Related Disorders, 3(4), 345–353. https://doi.org/10.1016/j.jocrd.2014.09.001
Flessner, C. A., Busch, A. M., Heideman, P. W., & Woods, D. W. (2008). Acceptance-enhanced behavior therapy (AEBT) for trichotillomania and chronic skin picking: exploring the effects of component sequencing. Behavior Modification, 32(5), 579–594. https://doi.org/10.1177/0145445507313800
Frydman, I., Vigne, P., Ferreira, G. M., Campos-Lima, A. L., Fontenelle, L. F., & Menezes, G. B. (2017). Comorbidity in obsessive-compulsive and related disorders. In J. S. Abramowitz, D. McKay, & E. A. Storch (Eds.), The Wiley handbook of obsessive compulsive disorders (pp. 1133–1151). Wiley.
Gallinat, C., Moessner, M., Haenssle, H. A., Winkler, J. K., Backenstrass, M., & Bauer, S. (2019). Help-seeking attitudes and experiences in individuals affected by skin picking. Journal of Obsessive-Compulsive and Related Disorders, 23, 100483.
Grant, J. (2016). Medications for body-focused repetitive behaviors. Retrieved from http://www.bfrb.org/component/content/article/3/186
Hannah, D. B., & Sternthal, B. (1984). Detecting and explaining the sleeper effect. Journal of Consumer Research, 11(2), 632–642.
Höffler, T. N., & Leutner, D. (2007). Instructional animation versus static pictures: A meta-analysis. Learning and Instruction, 17(6), 722–738. https://doi.org/10.1016/j.learninstruc.2007.09.013
Houghton, D. C., Alexander, J. R., Bauer, C. C., & Woods, D. W. (2018). Body-focused repetitive behaviors: More prevalent than once thought? Psychiatry Research, 270, 389–393. https://doi.org/10.1016/j.psychres.2018.10.002
Keuthen, N. J., Rothbaum, B. O., Fama, J., Altenburger, E., Falkenstein, M. J., Sprich, S. E., Kearns, M., Meunier, S., Jenike, M. A., & Welch, S. S. (2012). DBT-enhanced cognitive-behavioral treatment for trichotillomania: A randomized controlled trial. Journal of Behavioral Addictions, 1(3), 106–114. https://doi.org/10.1556/JBA.1.2012.003
Koehler, M. J., Yadav, A., Phillips, M. M., & Cavazos-Kottke, S. C. (2005). What is video good for? Examining how media and story genre interact. Journal of Educational Multimedia and Hypermedia, 14(3), 249–272.
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Lee, E. B., Homan, K. J., Morrison, K. L., Ong, C. W., Levin, M. E., & Twohig, M. P. (2020). Acceptance and commitment therapy for trichotillomania: A randomized controlled trial of adults and adolescents. Behavior Modification, 44(1), 70–91. https://doi.org/10.1177/0145445518794366
Lee, M. T., Mpavaenda, D. N., & Fineberg, N. A. (2019). Habit reversal therapy in obsessive compulsive related disorders: A systematic review of the evidence and CONSORT evaluation of randomized controlled trials. Frontiers in Behavioral Neuroscience, 13, 79. https://doi.org/10.3389/fnbeh.2019.00079
Mason, R. A., Ganz, J. B., Parker, R. I., Burke, M. D., & Camargo, S. P. (2012). Moderating factors of video-modeling with other as model: A meta-analysis of single-case studies. Research in Developmental Disabilities, 33(4), 1076–1086. https://doi.org/10.1016/j.ridd.2012.01.016
McGuire, J. F., Ung, D., Selles, R. R., Rahman, O., Lewin, A. B., Murphy, T. K., & Storch, E. A. (2014). Treating trichotillomania: A meta-analysis of treatment effects and moderators for behavior therapy and serotonin reuptake inhibitors. Journal of Psychiatric Research, 58, 76–83. https://doi.org/10.1016/j.jpsychires.2014.07.015
Moritz, S., Fricke, S., Treszl, A., & Wittekind, C. E. (2012). Do it yourself! Evaluation of self-help habit reversal training versus decoupling in pathological skin picking: A pilot study. Journal of Obsessive-Compulsive and Related Disorders, 1(1), 41–47. https://doi.org/10.1016/j.jocrd.2011.11.001
Moritz, S., Hoyer, L. & Schmotz, S. (in press). Two-year follow-up of habit reversal training and decoupling in a sample with body-focused repetitive behaviors. Cognitive Therapy and Research.
Moritz, S., Müller, K., & Schmotz, S. (2020a). Escaping the mouth-trap: Recovery from long-term pathological lip/cheek biting (morsicatio buccarum, cavitadaxia) using decoupling. Journal of Obsessive-Compulsive and Related Disorders. https://doi.org/10.1016/j.jocrd.2020.100530
Moritz, S., Rufer, M., & Schmotz, S. (2020b). Recovery from pathological skin picking and dermatodaxia using a revised decoupling protocol. Journal of Cosmetic Dermatology, 19(11), 3038–3040. https://doi.org/10.1111/jocd.13378
Moritz, S., Penney, D., Ahmed, K., & Schmotz, S. (2021). A head-to-head comparison of three self-help techniques to reduce body-focused repetitive behaviors. Behavior Modification. https://doi.org/10.1177/01454455211010707
Moritz, S., Penney, D., Bruhns, A., Weidinger, S., & Schmotz, S. (2023). Habit reversal training and variants of decoupling for use in body-focused repetitive behaviors: A randomized controlled trial. Cognitive Therapy and Research, 47(1), 109–122. https://doi.org/10.1007/s10608-022-10334-9
Moritz, S., & Rufer, M. (2011). Movement decoupling: A self-help intervention for the treatment of trichotillomania. Journal of Behavior Therapy and Experimental Psychiatry, 42(1), 74–80. https://doi.org/10.1016/j.jbtep.2010.07.001
Moritz, S., Treszl, A., & Rufer, M. (2011). A randomized controlled trial of a novel self-help technique for impulse control disorders: A study on nail-biting. Behavior Modification, 35(5), 468–485. https://doi.org/10.1177/0145445511409395
Noetel, M., Griffith, S., Delaney, O., Sanders, T., Parker, P., del Pozo Cruz, B., & Lonsdale, C. (2021). Video improves learning in higher education: A systematic review. Review of Educational Research, 91(2), 204–236. https://doi.org/10.3102/0034654321990713
Oliveira, S. E. H., Carvalho, H., & Esteves, F. (2016). Toward an understanding of the quality of life construct: Validity and reliability of the WHOQOL-Bref in a psychiatric sample. Psychiatry Research, 244, 37–44. https://doi.org/10.1016/j.psychres.2016.07.007
Ozcan, D., & Merdan, F. (2020). The effectiveness of video modelling for teaching daily life skills to children with autism spectrum disorder. International Journal of Learning and Teaching, 12(1), 42–54. https://doi.org/10.18844/ijlt.v12i1.4560
Roberts, S., O’Connor, K., Aardema, F., Bélanger, C., & Courchesne, C. (2016). The role of emotion regulation in body-focused repetitive behaviours. The Cognitive Behaviour Therapist, 9, e7. https://doi.org/10.1017/S1754470X16000039
Schmidt, J., Lamprecht, F., & Wittmann, W. W. (1989). Zufriedenheit mit der stationären Versorgung. Entwicklung eines Fragebogens und erste Validitätsuntersuchungen [Satisfaction with inpatient treatment; Satisfaction with inpatient care: Development of a questionnaire and first validity assessments]. Psychotherapie, Psychosomatik, Medizinische Psychologie, 39, 248–255.
Siddiqui, D., Qureshi, D., Marei, D., & Mahfouz, D. (2017). Onychophagia (nail biting): A body focused repetitive behavior due to psychiatric co-morbidity. Journal of Mood Disorders, 7(1), 48–49. https://doi.org/10.5455/jmood.20170204031431
Skurya, J., Jafferany, M., & Everett, G. J. (2020). Habit reversal therapy in the management of body focused repetitive behavior disorders. Dermatologic Therapy. https://doi.org/10.1111/dth.13811
Snorrason, I., Ólafsson, R. P., Flessner, C. A., Keuthen, N. J., Franklin, M. E., & Woods, D. W. (2012). The skin picking scale-revised: Factor structure and psychometric properties. Journal of Obsessive-Compulsive and Related Disorders, 1(2), 133–137. https://doi.org/10.1016/j.jocrd.2012.03.001
Solley, K., & Turner, C. (2018). Prevalence and correlates of clinically significant body-focused repetitive behaviors in a non-clinical sample. Comprehensive Psychiatry, 86, 9–18. https://doi.org/10.1016/j.comppsych.2018.06.014
Stockwell, B. R., Stockwell, M. S., Cennamo, M., & Jiang, E. (2015). Blended learning improves science education. Cell, 162(5), 933–936. https://doi.org/10.1016/j.cell.2015.08.009
Syring, M., Bohl, T., Kleinknecht, M., Kuntze, S., Rehm, M., & Schneider, J. (2015). Videos oder Texte in der Lehrerbildung? Effekte unterschiedlicher Medien auf die kognitive Belastung und die motivational-emotionalen Prozesse beim Lernen mit Fällen [Video or text in case-based teacher education?]. Zeitschrift Für Erziehungswissenschaft, 18(4), 667–685. https://doi.org/10.1007/s11618-015-0631-9
Teng, E. J., Woods, D. W., Twohig, M. P., & Marcks, B. A. (2002). Body-focused repetitive behavior problems: Prevalence in a nonreferred population and differences in perceived somatic activity. Behavior Modification, 26(3), 340–360. https://doi.org/10.1177/0145445502026003003
The WHOQOL Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551–558. https://doi.org/10.1017/S0033291798006667
Tucker, B. T. P., Woods, D. W., Flessner, C. A., Franklin, S. A., & Franklin, M. E. (2011). The skin picking impact project: Phenomenology, interference, and treatment utilization of pathological skin picking in a population-based sample. Journal of Anxiety Disorders, 25(1), 88–95. https://doi.org/10.1016/j.janxdis.2010.08.007
Wang, W.-C., Yao, G., Tsai, Y.-J., Wang, J.-D., & Hsieh, C.-L. (2006). Validating, improving reliability, and estimating correlation of the four subscales in the WHOQOL-BREF using multidimensional rasch analysis. Quality of Life Research, 15(4), 607–620. https://doi.org/10.1007/s11136-005-4365-7
Weingarden, H., & Renshaw, K. D. (2015). Shame in the obsessive compulsive related disorders: A conceptual review. Journal of Affective Disorders, 171, 74–84. https://doi.org/10.1016/j.jad.2014.09.010
Woods, D. W., Wetterneck, C. T., & Flessner, C. A. (2006). A controlled evaluation of acceptance and commitment therapy plus habit reversal for trichotillomania. Behaviour Research and Therapy, 44(5), 639–656. https://doi.org/10.1016/j.brat.2005.05.006
Acknowledgements
We would like to thank all who participated in this study. The authors received no financial support for the research, authorship, and/or publication of this article.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors have not disclosed any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interest
The authors report no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Moritz, S., Weidinger, S. & Schmotz, S. ‘Free from BFRB’: Efficacy of Self-Help Interventions for Body-Focused Repetitive Behaviors Conveyed via Manual or Video. J Contemp Psychother 54, 103–112 (2024). https://doi.org/10.1007/s10879-023-09609-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10879-023-09609-3