
Abstract
Background
IgA deficiency (IGAD) is the most common primary antibody deficiency. Although many affected individuals have no apparent symptom, selected patients suffer from recurrent mucosal infections, allergies, and autoimmune diseases. We aimed to investigate the clinical features in relation to immune function of Iranian patients with symptomatic IGAD.
Methods
Thirty-seven patients (21 male and 16 female), aged 4–32 years, were evaluated in this study. Patients were followed for a total of 131 patient years with a mean follow-up of 3.5 years per patient.
Results
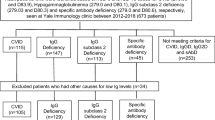
The most prevalent presentations were recurrent infections occurring in 27 subjects, followed by allergy in eight cases and autoimmunity in two patients. However, during the follow-up period, 35 patients developed infections in respiratory and gastrointestinal tracts, necessitating medical care. Apart from infections, allergy was the most frequent complaint (31 cases); the major features were asthma, atopic dermatitis, and allergic rhinoconjunctivitis. Autoimmune diseases were documented in ten cases; thyroiditis was the most common. In 31 patients who received unconjugated pneumococcal polyvalent vaccine, antibody response against polysaccharide antigen was measured before and 28 days after vaccination. One fourth of vaccinated patients were hyporesponsive to vaccine; four of these patients developed bronchiectasis. The patients with IGAD were classified into two groups: group 1 (14 cases) consisted of patients with IGAD and other associated immune defects, such as immunoglobulin G (IgG) subclass deficiency and defective specific antibody production. Group 2 (23 cases) had isolated IGAD without other immunological abnormalities. There was a significantly increased number of lower respiratory tract infections in group 1 compared with group 2 (P = 0.006). Moreover, four patients of group 1 had bronchiectasis whereas none of the patients in group 2 developed this complication (P = 0.015).
Conclusion
Subclassification of IGAD regarding the existence of associated immune defects is useful in terms of morbidity and planning for medical care. IgA-deficient patients with concomitant immune defects such as defects in specific antibody production have higher rates of recurrent infections and bronchiectasis, which necessitates more effective monitoring.

Similar content being viewed by others


References
Hammarstrom L, Vorechovsky I, Webster D. Selective IgA deficiency (SIgAD) and common variable immunodeficiency (CVID). Clin Exp Immunol. 2000;120(2):225–31. doi:10.1046/j.1365-2249.2000.01131.x.
Bonilla FA, Bernstein IL, Khan DA, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol. 2005;94(5):S1–63.
Conley ME, Notarangelo LD, Etzioni A. Diagnostic criteria for primary immunodeficiencies. Representing PAGID (Pan-American Group for Immunodeficiency) and ESID (European Society for Immunodeficiencies). Clin Immunol. 1999;93(3):190–7. doi:10.1006/clim.1999.4799.
al-Attas RA, Rahi AH. Primary antibody deficiency in Arabs: first report from eastern Saudi Arabia. J Clin Immunol. 1998;18(5):368–71. doi:10.1023/A:1023247117133.
Cunningham-Rundles C. Physiology of IgA and IgA deficiency. J Clin Immunol. 2001;21(5):303–9. doi:10.1023/A:1012241117984.
Kanoh T, Mizumoto T, Yasuda N, et al. Selective IgA deficiency in Japanese blood donors: frequency and statistical analysis. Vox Sang. 1986;50(2):81–6.
Schaffer FM, Monteiro RC, Volanakis JE, Cooper MD. IgA deficiency. Immunodefic Rev. 1991;3(1):15–44.
Burrows PD, Cooper MD. IgA deficiency. Adv Immunol. 1997;65:245–76. doi:10.1016/S0065-2776(08)60744-0.
Hanson LA, Bjorkander J, Carlsson B, Roberton D, Soderstrom T. The heterogeneity of IgA deficiency. J Clin Immunol. 1988;8(3):159–62. doi:10.1007/BF00917561.
Burgio GR, Duse M, Monafo V, Ascione A, Nespoli L. Selective IgA deficiency: clinical and immunological evaluation of 50 pediatric patients. Eur J Pediatr. 1980;133(2):101–6. doi:10.1007/BF00441577.
Crabbe PA, Heremans JF. The significance of local IgA in the physiology of the intestinal mucosa. Folia Med Neerl. 1969;12(3):100–6.
Heneghan MA, Stevens FM, Cryan EM, Warner RH, McCarthy CF. Celiac sprue and immunodeficiency states: a 25-year review. J Clin Gastroenterol. 1997;25(2):421–5. doi:10.1097/00004836-199709000-00004.
Sloper KS, Brook CG, Kingston D, Pearson JR, Shiner M. Eczema and atopy in early childhood: low IgA plasma cell counts in the jejunal mucosa. Arch Dis Child. 1981;56(12):939–42.
Edwards E, Razvi S, Cunningham-Rundles C. IgA deficiency: clinical correlates and responses to pneumococcal vaccine. Clin Immunol. 2004;111(1):93–7. doi:10.1016/j.clim.2003.12.005.
Strober W, Sneller MC. IgA deficiency. Ann Allergy. 1991;66(5):363–75.
Wernette CM, Frasch CE, Madore D, et al. Enzyme-linked immunosorbent assay for quantitation of human antibodies to pneumococcal polysaccharides. Clin Diagn Lab Immunol. 2003;10(4):514–9. doi:10.1128/CDLI.10.4.514-519.2003.
Vendrell M, de Gracia J, Rodrigo MJ, et al. Antibody production deficiency with normal IgG levels in bronchiectasis of unknown etiology. Chest 2005;127(1):197–204. doi:10.1378/chest.127.1.197.
Standardization of spirometry-1987 update. Statement of the American Thoracic Society. Am Rev Respir Dis. 1987;136(5):1285–98.
Aghamohammadi A, Mohammadi J, Parvaneh N, Rezaei N, Moin M, Espanol T, et al. Progression of selective IgA deficiency to common variable immunodeficiency. Int Arch Allergy Immunol 2008;147(2):87–92. doi:10.1159/000135694.
Schroeder HW Jr, Zhu ZB, March RE, et al. Susceptibility locus for IgA deficiency and common variable immunodeficiency in the HLA-DR3, -B8, -A1 haplotypes. Mol Med. 1998;4(2):72–86.
Castigli E, Wilson SA, Garibyan L, et al. TACI is mutant in common variable immunodeficiency and IgA deficiency. Nat Genet 2005;37(8):829–34. doi:10.1038/ng1601.
Salzer U, Chapel HM, Webster AD, et al. Mutations in TNFRSF13B encoding TACI are associated with common variable immunodeficiency in humans. Nat Genet. 2005;37(8):820–8. doi:10.1038/ng1600.
Hammarström LSC. Genetic approach to common variable immunodeficiency and IgA deficiency. In: Ochs HDSC, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 313–25.
Rezaei N, Aghamohammadi A, Moin M, Pourpak Z, Movahedi M, Gharagozlou M, et al. Frequency and clinical manifestations of patients with primary immunodeficiency disorders in Iran: update from the Iranian Primary Immunodeficiency Registry. J Clin Immunol. 2006;26(6):519–32. doi:10.1007/s10875-006-9047-x.
Saghafi S, Pourpak Z, Aghamohammadi A, Pourfathollah AA, Samadian A, Farghadan M, et al. Selective immunoglobulin a deficiency in Iranian blood donors; prevalence, laboratory and clinical findings. Iran J Allergy Asthma Immunol. 2008;7(3):157–62.
Ozkan H, Atlihan F, Genel F, Targan S, Gunvar T. IgA and/or IgG subclass deficiency in children with recurrent respiratory infections and its relationship with chronic pulmonary damage. J Investig Allergol Clin Immunol. 2005;15(1):69–74.
Stead A, Douglas JG, Broadfoot CJ, Kaminski ER, Herriot R. Humoral immunity and bronchiectasis. Clin Exp Immunol. 2002;130(2):325–30. doi:10.1046/j.1365-2249.2002.01974.x.
Tabatabaie P, Aghamohammadi A, Mamishi S, Isaeian A, Heidari G, Abdollahzade S, MirSaeid Ghazi B, Yeganeh M, Cheraghi T, Abolhasani H, Saghafi S, Alizadeh H, Anaraki MR, et al. Evaluation of humoral immune function in patients with bronchiectasis. Iran J Allergy Asthma Immunol. 2008;7(2):69–77.
Stiehm RE. The four most common pediatric immunodeficiencies. Adv Exp Med Biol. 2007;601:15–26.
Golshan M, Mohamad-Zadeh Z, Zahedi-Nejad N, Rostam-Poor B. Prevalence of asthma and related symptoms in primary school children of Isfahan, Iran, in 1998. Asian Pac J Allergy Immunol. 2001;19(3):163–70.
Golshan M, Mohammad-Zadeh Z, Khanlar-Pour A, Iran-Pour R. Prevalence of asthma and related symptoms in junior high school children in Isfahan, Iran. Monaldi Arch Chest Dis. 2002;57(1):19–24.
Miri S, Farid R, Akbari H, Amin R. Prevalence of allergic rhinitis and nasal smear eosinophilia in 11- to 15 yr-old children in Shiraz. Pediatr Allergy Immunol. 2006;17(7):519–23. doi:10.1111/j.1399-3038.2006.00424.x.
Mirsaid Ghazi B, Imamzadehgan R, Aghamohammadi A, Darakhshan Davari R, Rezaei N. Frequency of allergic rhinitis in school-age children (7–18 Years) in Tehran. Iran J Allergy Asthma Immunol. 2003;2(4):181–4.
Ammann AJ, Hong R. Selective IgA deficiency: presentation of 30 cases and a review of the literature. Medicine 1971;60:223–36. doi:10.1097/00005792-197105000-00004.
Woof JM, Kerr MA. The function of immunoglobulin A in immunity. J Pathol. 2006;208(2):270–82. doi:10.1002/path.1877.
Bjorkander J, Bake B, Oxelius VA, Hanson LA. Impaired lung function in patients with IgA deficiency and low levels of IgG2 or IgG3. N Engl J Med. 1985;313(12):720–4.
Bossuyt X, Moens L, Van Hoeyveld E, et al. Coexistence of (partial) immune defects and risk of recurrent respiratory infections. Clin Chem. 2007;53(1):124–30. doi:10.1373/clinchem.2007.075861.
French MA, Denis KA, Dawkins R, Peter JB. Severity of infections in IgA deficiency: correlation with decreased serum antibodies to pneumococcal polysaccharides and decreased serum IgG2 and/or IgG4. Clin Exp Immunol. 1995;100(1):47–53.
Oxelius VA, Laurell AB, Lindquist B, et al. IgG subclasses in selective IgA deficiency: importance of IgG2-IgA deficiency. N Engl J Med. 1981;304(24):1476–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Aghamohammadi, A., Cheraghi, T., Gharagozlou, M. et al. IgA Deficiency: Correlation Between Clinical and Immunological Phenotypes. J Clin Immunol 29, 130–136 (2009). https://doi.org/10.1007/s10875-008-9229-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-008-9229-9