
Abstract
Background
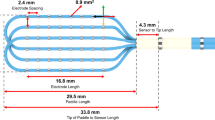
Defining diastolic slow-conduction channels within the borderzone (BZ) of scar-dependent re-entrant ventricular tachycardia (VT) is key for effective mapping and ablation strategies. Understanding wavefront propagation is driving advances in high-density (HD) mapping. The newly developed Advisor™ HD Grid Mapping Catheter (HD GRID) has equidistant spacing of 16, 1 mm electrodes in a 4 × 4 3 mm interspaced arrangement allowing bipolar recordings along and uniquely across the splines (orthogonal vector) to facilitate substrate mapping in a WAVE configuration (WAVE). The purpose of this study was to determine the relative importance of the WAVE configuration compared to the STANDARD linear-only bipolar configuration (STANDARD) in defining VT substrate.
Methods
Thirteen patients underwent VT ablation at our institution. In all cases, a substrate map was constructed with the HD GRID in the WAVE configuration (conWAVE) to guide ablation strategy. At the end of the procedure, the voltage map was remapped in the STANDARD configuration (conSTANDARD) using the turbo-map function. Detailed post-hoc analysis of the WAVE and STANDARD maps was performed blinded to the configuration. Quantification of total scar area, BZ and dense scar area with assessment of conduction channels (CC) was performed.
Results
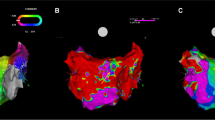
The substrate maps conSTANDARD vs conWAVE showed statistically significant differences in the total scar area (56 ± 32 cm2 vs 51 ± 30 cm2; p = 0.035), dense scar area (36 ± 25 cm2 vs 29 ± 22 cm2; p = 0.002) and number of CC (3.3 ± 1.6 vs 4.8 ± 2.5; p = 0.026). conWAVE collected more points than the conSTANDARD settings (p = 0.001); however, it used fewer points in map construction (p = 0.023).
Conclusions
The multipolar Advisor™ HD Grid Mapping Catheter in conWAVE provides more efficient point acquisition and greater VT substrate definition of the borderzone particularly at the low-voltage range compared to conSTANDARD. This greater resolution within the low-voltage range facilitated CC definition and quantification within the scar, which is essential in guiding the ablation strategy.




Similar content being viewed by others

References
Stevenson WG, Khan H, Sager P, Saxon LA, Middlekauff HR, Natterson PD, et al. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Circulation. 1993;88:1647–70.
Volkmer M, Ouyang F, Deger F, Ernst S, Goya M, Bänsch D, et al. Substrate mapping vs. tachycardia mapping using CARTO in patients with coronary artery disease and ventricular tachycardia: impact on outcome of catheter ablation. Europace. 2006;8:968–76.
Di Biase L, Santangeli P, Burkhardt DJ, Bai R, Mohanty P, Carbucicchio C, et al. Endo-epicardial homogenization of the scar versus limited substrate ablation for the treatment of electrical storms in patients with ischemic cardiomyopathy. J Am Coll Cardiol. 2012;60:132–41.
Proietti R, Essebag V, Beardsall J, Hache P, Pantano A, Wulffhart Z, et al. Substrate-guided ablation of haemodynamically tolerated and untolerated ventricular tachycardia in patients with structural heart disease: effect of cardiomyopathy type and acute success on long-term outcome. Europace. 2014:1–7.
Di Biase L, Burkhardt JD, Lakkireddy D, Carbucicchio C, Mohanty S, Mohanty P, et al. Ablation of stable VTs versus substrate ablation in ischemic cardiomyopathy: the VISTA randomized multicenter trial. J Am Coll Cardiol. 2015;66:2872–82.
Mountantonakis SE, Park RE, Frankel DS, Hutchinson MD, Dixit S, Cooper J, et al. Relationship between voltage map ‘channels’ and the location of critical isthmus sites in patients with post-infarction cardiomyopathy and ventricular tachycardia. J Am Coll Cardiol. 2013;61:2088–95.
Pedersen CT, Kay GN, Kalman J, Borggrefe M, Della-Bella P, Dickfeld T, et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm. 2014;11:e166–96.
Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation. 2000;101:1288–96.
Proietti R, Roux J-F, Essebag V. Recent advances in ablation of ventricular tachycardia associated with structural heart disease: overcoming the challenges of functional and fixed barriers. Curr Opin Cardiol. 2016;31:64–71.
de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, et al. Slow conduction in the infarcted human heart. ‘Zigzag’ course of activation. Circulation. 1993;88:915–26.
De Bakker JMT, Wittkampf FHM. The pathophysiologic basis of fractionated and complex electrograms and the impact of recording techniques on their detection and interpretation. Circ Arrhythm Electrophysiol. 2010;3:204–13.
Bellmann B, Lüker J, Steven D, Sultan A. First epicardial mapping of the left ventricle using the Advisor™ HD grid catheter. J Interv Card Electrophysiol. 2018;53:103–4.
Sosa E, Scanavacca M, d’Avila A, Oliveira F, Ramires JAF. Nonsurgical transthoracic epicardial catheter ablation to treat recurrent ventricular tachycardia occurring late after myocardial infarction. J Am Coll Cardiol. 2000;35:1442–9.
Takigawa M, Relan J, Martin R, Kim S, Kitamura T, Frontera A, et al. Effect of bipolar electrode orientation on local electrogram properties. Heart Rhythm. 2018;15:1853–61.
Mbbs CY, Hsen V, Mbbs T, Cheok K, Wong K. Pulmonary vein reconnection mapping with Advisor HD Grid demonstrating local EGM which were not visible on Tacticath ablation catheter. J Arrhythmia. 2018:152–4.
Berruezo A, Fernández-Armenta J, Andreu D, Penela D, Herczku C, Evertz R, et al. Scar dechanneling: a new method for scar-related left ventricular tachycardia substrate ablation. Circ Arrhythm Electrophysiol. 2015;8(2):326–36 CIRCEP—114.
Brunckhorst CB, Delacretaz E, Soejima K, Maisel WH, Friedman PL, Stevenson WG. Impact of changing activation sequence on bipolar electrogram amplitude for voltage mapping of left ventricular infarcts causing ventricular tachycardia. J Interv Card Electrophysiol. 2005;12:137–41.
Tung R, Josephson ME, Bradfield JS, Shivkumar K. Directional influences of ventricular activation on myocardial scar characterization: voltage mapping with multiple wavefronts during ventricular tachycardia ablation. Circ Arrhythm Electrophysiol. 2016;9:1–11.
Dhanjal TS, Lellouche N, von Ruhland CJ, Abehsira G, Edwards DH, Dubois-Randé J-L, et al. Massive accumulation of myofibroblasts in the critical isthmus is associated with ventricular tachycardia inducibility in post-infarct swine heart. JACC Clin Electrophysiol. 2017;3:703–14.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Proietti, R., Adlan, A.M., Dowd, R. et al. Enhanced ventricular tachycardia substrate resolution with a novel omnipolar high-density mapping catheter: the omnimapping study. J Interv Card Electrophysiol 58, 355–362 (2020). https://doi.org/10.1007/s10840-019-00625-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-019-00625-9